Download
1 / 39
680 likes | 1.45k Views
Comprehensive Video EEG monitoring. JWM Neurology Kate Kobza, MD August 2006. Why do we need it?. Limitations of routine EEG:. Limited sampling An EEG is a sampling of brain activity occurring at the time of the recording

E N D
Comprehensive Video EEG monitoring JWM Neurology Kate Kobza, MD August 2006
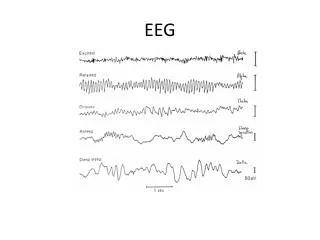
Limitations of routine EEG: • Limited sampling • An EEG is a sampling of brain activity occurring at the time of the recording • Seizures and spells are paroxysmal and may be missed on a short study • No video to correlate patient behavior with suspicious EEG changes
Limitations of routine EEG: • Yield of a single routine scalp EEG is 50% • Certain artifacts and normal variants can be confused with epileptiform discharges • Some EEG abnormalities do not have a close correlation with clinical seizures
Limitations of routine EEG: • Pathophysiologically – epileptic seizures are characterized by an excessive, disorderly, neuronal discharge • An EEG study may disclose epileptiform abnormalities which have a high correlation with occurrence of epileptic seizures • The only way to definitively prove epilepsy is to record a seizure
Methodology • EEG electrodes are attached to the scalp with glue • ECG electrodes are placed • Patient is moved to a room with video monitoring • Patient and family are given an alarm to push with any spell • Trained nurses and staff respond to alarms to observe patient and treat if necessary
Methodology • Miscellaneous options: • Antiepileptic medications may be discontinued or decreased • Known inducers of events may be performed • Sleep deprivation • Suggestion (important in nonepileptic events) • Extra electrodes may be added • Sphenoidal • Foramen ovale
Methodology • Multi-channel long term EEG recording with split screen video recording • Digital storage of EEG and video data that can be reviewed later • Performed under close monitoring of trained technologists and nurses • Study is reviewed by a trained neurologist or epileptologist
Outpatient settings • Represents a partially controlled environment • Useful for: • Minor or non-convulsive seizures • Diagnostic purposes only • Benefits: • Less costly • Drawbacks: • Invasive electrodes not possible • No medication withdrawal possible
Inpatient settings • Completely controlled environment • Useful for: • Major or convulsive seizures • Medication withdrawal possible • Benefits: • Other tests: Blood sugars, SPECT possible • Inducers can be used, if present • Invasive electrode monitoring possible • Intracranial EEG possible • Drawbacks: • Expensive
Primarily neurologists order video EEG studies • Video EEG can be ordered on infants, children, and adults
Common indications: • Follow up of borderline or nonconclusive routine EEGs • Diagnosis of recurrent spells • Classification of seizure type • Quantification of interictal epileptiform activity • Preoperative evaluation of surgical candidates • Evaluation of patient in coma as treatments for status epilepticus
Follow-up borderline EEG • Allows for prolonged collection of digital EEG • Areas of uncertainty (i.e. artifact vs. abnormality) can be correlated with video material for clarification
Aids in diagnosis of spells: • Causes other than epileptic seizures: • Syncope • Sleep apnea • Periodic movements of sleep • Non-epileptic seizures • Breath-holding spells • Migraine
Other uses: • Characterization or any repetitive or stereotyped behavior • autonomic changes in infants • repetitive behaviors in the ICU setting • unexplained nocturnal events
Characterization of seizures • Accurate diagnosis and classification of seizures is essential for proper therapeutic intervention • Medication choices are driven by seizure classification
Classification of seizure types • Generalized • Absence • Generalized tonic, clonic, or atonic • Myoclonic • Partial onset • Simple or complex • Secondary generalization • Non epileptic
Examples of seizure types • Complex partial • Generalized tonic-clonic • Nonepileptic
Diagnosis of non-epileptic events: Pseudoseizures • Studies1 have shown that 22% of patients with medically intractable seizures studied by video EEG monitoring had nonepileptic events • Approximately 1/3 of patients studied at video monitoring centers have nonepileptic events • The majority of patients with nonepileptic events have been inappropriately treated with antiepileptic medications for years • 1 Matson et al.
Nonepileptic events • Video EEG monitoring provides evidence to support medication choices • Allows safe discontinuation of antiepileptic drugs • Information can be used when discussing a diagnosis of pseudoseizure with patients • Many patients are relieved by diagnosis • Many others are doubtful as they have been told for many years that they have epilepsy • This is used to as a treatment modality
Nonepileptic events • Majority of patients with nonepileptic events also experience epileptic seizures • Video EEG can quantitate frequency of each type • Aids in education of family members about clinical differences • Avoid abuse of resources • Limit health provider calls • Avoid abuse (overuse) of antiepileptic drugs
Quantification of interictal epileptiform activity • Quantify the number of seizures per day • Helpful for: • Absence seizures • Helpful in decision to stop medications • Nonconvulsive seizures • Document efficacy of suppressive medications
Localization of epileptogenic focus • Useful in patients with intractable epilepsy as part of a presurgical evaluation • Focus of study is to correlate EEG findings with lesion on MRI
Preoperative evaluation of surgical candidates • Usually for intractable temporal or extra-temporal epilepsy • Can be performed with sphenoidal or foramen ovale electrodes • Subdural grid placements can be used in conjunction with a neurosurgeon
Evaluation of patient in coma as treatments for status epilepticus
Status epilepticus • Patients often demonstate continued subclinicalseizure discharges after the clinical behaviors have cease • EEG monitoring is necessary in all patients in drug induced coma as a treatment for status epilepticus • Need to document burst suppression pattern induced by meds
Long term EEG monitoring: Other uses • Intraoperatively: • Functional stimulation during resections • Intraoperative surface EEG monitoring • carotid endarterectomy
Other monitoring modalities: • Digital ambulatory monitoring • Patient wears a digital EEG recorder home • Records 24 hours of digital EEG • Patient records symptoms in a diary
In Summary:Video EEG monitoring • Captured 50-96% of epileptic and nonepileptic events (Legatt AD and Ebersole JS, 1998). • Established a diagnosis in 88-95% (Legatt AD and Ebersole JS, 1998). • Improved outcome in 30-74% of patients (Legatt AD and Ebersole JS, 1998).
St. Vincent Hospital • Routine EEG – outpatient or inpatient • Ambulatory EEG – 24 hour outpatient study • Video EEG monitoring • 3 adult rooms (hardwired) • 1 portable unit (adult or pediatric) • 1 ICU monitoring room