Download
1 / 60
600 likes | 616 Views
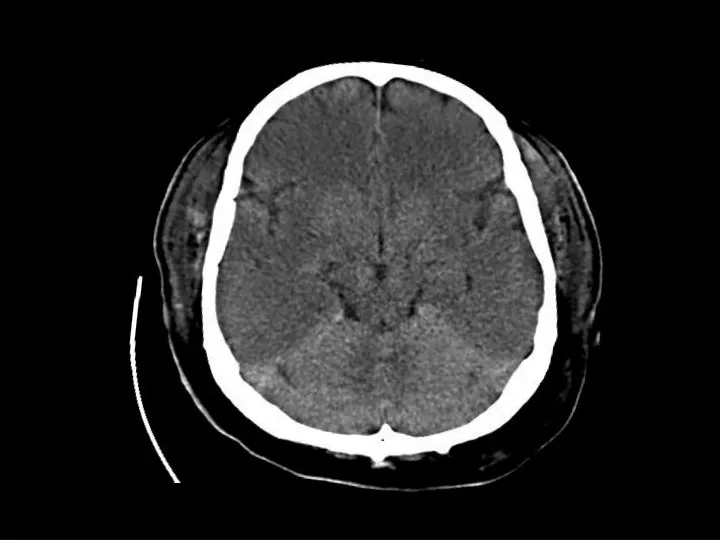
Anoxic Brain Injury. Findings: Hypodense cerebral hemispheres with effacement of cortical gyri Relative sparing of cerrebellum Due to global insult: Profound hypotension Carbon monoxide poisoning MRI findings: Dense basal ganglia. Synovial Cyst of the Lumbar Spine. Findings:

E N D
Anoxic Brain Injury • Findings: • Hypodense cerebral hemispheres with effacement of cortical gyri • Relative sparing of cerrebellum • Due to global insult: • Profound hypotension • Carbon monoxide poisoning • MRI findings: • Dense basal ganglia
Synovial Cyst ofthe Lumbar Spine • Findings: • Low T1, high T2 extradural lesion contiguous with the facet joint • Surrounding enhancement • Mass effect • Associated with degenerated joints – 75% at L4-5 • Typically posterolateral • Contents variable – clear fluid, calcium, hemorrhage • ddx: • Migrated herniated disc • Perineural cyst (close to nerve root) • Schwannoma (low sig capsule) • Hematoma
Diffuse Axonal Injury • Findings: • Diffuse brain swelling • Focal punctate hemorrhage scattered in the white matter, corpus callosum, and brain stem • Right subgaleal hematoma • Due to diffuse shearing injury, sudden deceleration (MVA) • MRI findings: • Hemorrhage best seen on GRE sequence
PCOM aneurysm clippinganterior choroidal artery infarct • Findings: • Recent right pterional surgery • Aneurysm clips at PCOM • Low attn at the right genu of internal capsule = infarct • Pt wakes up with hemiparesis • Devastating complication of PCOM aneurysm clipping
Cavernoma of the Spine • Findings: • “popcorn-like” intramedullary lesion in the conus • T2: faint high signal • T2: high signal centrally, dark rim, and high signal peripherally • a.k.a. Cavernoma, cavernous hemangioma, and capillary hemangioma • Congenital abnormal cluster of capillaries and venules that periodically bleed • Signal characteristics are that of blood in different stages • Angiographically occult • Look for multiple lesions on GRE
Inverting Papilloma • Findings: • Soft tissue mass involving the maxillary sinus and nasal cavity • Expansion of sinus with bone remodeling, not destruction • Benign tumors of the lateral nasal wall which extend in to the maxillary and/or ethmoid • Can homogeneously enhance • Look for widening of the infundibulum • ddx: • Antrochoanal polyp • Mucocele
Nerve root avulsion and pseudomeningocele • Findings: • Abnormal high T2 signal dumbbell-shaped lesion in a high thoracic neural foramen • Mass effect on thecal sac • Large high T2 collection in the adjacent soft tissues • A result of major trauma • Disruption of the meninges and spill of CSF into surrounding tissues • Focal collection at the nerve root may appear as a discrete mass and displace thecal sac
Herpes Encephalitis • Findings • Bilateral temporal lobe FLAIR signal (post-seizure edema) • HSV 2 in neonates • HSV 1 in adults • latent infection in the Gasserian ganglion (CN V) • predilection for the limbic syste, cingulate gyrus, and subfrontal region • late stage becomes bilateral, hemorrhage
Cortical Laminar Necrosis • Findings: • Cortical calcification of the posterior right MCA territory • Due to infarction • If global, think of hypoxic injury, hypoglycemia, or encephalitis
Primary Intracerebral Lymphoma • Findings: • T2 bright lesion in the left frontal lobe and basal ganglia • Crosses both gray and white matter • Some mass effect • No significant enhancement • An unusual lesion in the non-HIV/immunosuppred population • ddx: • Low –grade glioma
Spinal Sarcoid • Findings: • Iso T1, hyper T2, enhancing lesion of cervical spinal cord • No significant cord expansion • Idiopathic system disease characterized by non-caseating granulomas • Young, black women • Image the brain, check CXR • ddx: • Transverse myelitis • Demyelinating dz (MS) • Primary cord tumor (ependymoma, astrocytoma) • Met (uncommon)
Septic Sacroiliitis • Findings: • Low T1, high T2 abnormality in the right SI joint • Uncommon infection usually due to strep • ddx: • Unilateral • Gout • Osteoarthritis • Bilateral & symmetric • Ankylosing spondylitis • Inflammatory Bowel Dz • Bilateral & asymmetric • Psoriatic arthritis • Reiter syndrome • Rheumatoid
MCA hemorrhagic infarction • Findings: • Large hemorrhage in the right insula • Much surrounding edema • Some mass effect • Due to M1 segment embolus affecting lateral lenticulostriate arteries • ddx: • Hypertensive hemorrhage (usually little or no edema) • Underlying tumor or AVM (need angio to confirm)
Spinal Multiple Sclerosis • Findings: • Cord edema • Flame-shaped intramedullary enhancement • No significant cord expansion • Image the brain, check the optic nerves • ddx: • Transverse myelitis • Sarcoid • Primary cord tumor • Mets
Sacral Insufficiency Fracture • Findings: • High T2 signal in the left sacral ala crossing the midline and involving the right side • Normal stress on abnormal bone (usually osteoporosis) • Pts can have non-specific back or hip pain • Plain films show lucency, then sclerosis • Bone scan show classic “Honda sign” • ddx: • acute fractures • metastases
Lymphoepithelial cysts in HIV • Findings: • Enlarged parotid glands containing innumerable small cystic lesions • Manifestation in HIV, unclear etiology • Soft, non-tender enlarged glands • ddx: • Sjogren’s syndrome • Warthin’s tumors
TB meningitis • Findings: • High attenuation of the cerebellar folia • Look for the primary site (lungs); usually a post-primary infection • Long and protracted illness rather an typical sx of acute bacterial meningitis • Look for BASAL involvement • ddx: • Carcinomatous meningitis • Sarcoidosis • Lymphoma • Subarachnoid blood
Anaplastic Astrocytoma • Findings: • Ill-defined T2 signal abnormality involving both gray and white matter • Crosses vascular territories and into corpus callosum • Mass effect on ventricle • The most common primary brain tumor • Tumor margin likely beyond T2 boundary • Don’t let lack of enchancement fool you!
Spinal Dural AVF • Findings: • Expanded, edematous cord • Multiple extramedullary high signal foci • Direct AV communication leads to venous hypertension, cord congestion, and infarction • Extramedullary AVFs DO NOT bleed • Intramedullary AVMs have a nidus, present in kids as acute paresis due to spontaneous hemorrhage • ddx: • Leptomeningeal carcinomatosis
Rathke’s Cleft Cyst • Findings: • High T1 & T2 slightly expansile sellar lesion • Displaces normal pituitary tissue • Non-neoplastic remnants of Rathke’s pouch • majority are asymptomatic, symptoms include visual defects, pit insufficiency, headaches • Can be high or low T1 but always high T2 • Ddx: • Arachnoid cyst • Epidermoid • Pituitray adenoma • craniopharyngioma
Carotid body paraganglioma • Findings: • Intensely enhancing mass in the carotid sheath that splays the internal and external carotid arteries • ddx: • Glomus vagali • Carotid aneurysm
Glioblastoma multifome • Findings: • Aggressive intra-axial enchancing mass lesion with central necrosis • ddx: • Abscess • Tumafactive MS