Download
1 / 56
560 likes | 738 Views
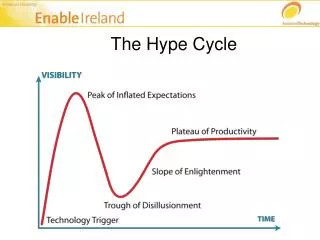
Clinical Decision Support Lecture Brief History and State of the Art of Clinical Decision Support and relation to Terminology and Electronic Healthcare Records (EHRs) Available at http://www.cs.man.ac.uk/~rector/modules/cds/Notes-1-HI-general-cds-2006.ppt. The Hype of the Time. Guidelines

E N D
Clinical Decision Support Lecture Brief History and State of the Art of Clinical Decision Support and relation to Terminology and Electronic Healthcare Records (EHRs)Available at http://www.cs.man.ac.uk/~rector/modules/cds/Notes-1-HI-general-cds-2006.ppt www.cs.man.ac.uk/ai/modules/cds
The Hype of the Time • Guidelines • Evidence Based Medicine • Clinical Errors (reducing) • Improving prescribing practice • Reducing adverse drug reactions • Protocols • Knowledge Management • ... www.cs.man.ac.uk/ai/modules/cds
Clinical Judgement and Clinical Errors • To Err is Human http://www.nap.edu/books/0309068371/html/ • Supporting a Humanly Impossible Task http://www.cs.man.ac.uk/~rector/papers/Humanly-Impossible-Task.pdf • Johnson Articles - see resourceshttp://www.cs.man.ac.uk/~rector/modules/cds/cds_links.htm(NB some links may be broken because of University merger) • OpenClinical Web sitehttp://www.openclinical.org/ • OpenEHR web sitehttp://www.openehr.org www.cs.man.ac.uk/ai/modules/cds
Computer Aided Decision Support Works (sometimes) • Evidence of effectiveness growing • 25 years since Clem McDonald’s Protocol-based computer reminders, the quality of care and the non-perfectability of man • Use still limited • Meta studies and reviews a decade old • Elson R E and Connelly D P (1995). Computerized patient records in primary care: Their role in mediating guideline-driven physician behaviour change. Archives of Family Medicine 4: 698-705. • Grimshaw J and Russell I (1993). Effect of clinical guidelines on medical practice: a systematic review of rigorous evaluations. Lancet 342: 1317-1322. • Johnston M, Langton K, Haynes R and Mathieu A (1994). Effects of computer-based clinical decision support systems on clinical performance and patient outcome. A critical appraisal of research. Archives of Internal Medicine 120: 135-142. www.cs.man.ac.uk/ai/modules/cds
Important Recent Study • Cristina Tural, Lidia Ruiz , Christopher Holtzer, Jonathan Schapiro, Pompeyo Viciana, Juan Gonzàlez , Pere Domingo,Charles Bouche, C. Rey-Jol. BonaventuraClotet and the Havana Study Group (2002) Clinical utility of HIV-1 genotyping and expert advice: Havana trial, AIDS 16(2): 209-215 www.cs.man.ac.uk/ai/modules/cds
Types of Decision Support: Information Tasks • Informative • Guidelines e.g. eBNF, BMJ Clinical Evidence,... • Literature search - DxPlain • Information structuring • intelligent records (EPRs) • PEN&PAD, Medcin vocabulary, ... • Triggers and warnings • MLMs, McDonald’s original work, HELP, ... • Critiquing - Perry Miller • Advising www.cs.man.ac.uk/ai/modules/cds
Types of Decision Support: Clinical Tasks • Management Protocols(often effective, Johnston et. al 1994) • Prescribing • Protocol based care • Oncocin, T-Helper, etc. • Referral • Diagnosis(rarely effective, Johnston et. Al 1994) • Mycin • Internist I • Knowledge Couplers www.cs.man.ac.uk/ai/modules/cds
Reasons for success and failure(1) • Understanding of problem • Meeting real and recognised needs • Forsythe D E (1992). Using ethnography to build a working system: rethinking basic design assumptions. Sixteenth Annual Symposium on Computer Applications in Medical Care (SCAMC-92), Baltimore, MD, Baltimore, MD: 505-509. • Meeting them effectively • “The user is always right… but the user is usually wrong” • The technology is still crude at best • Implementing it successfully www.cs.man.ac.uk/ai/modules/cds
Reasons for success and failure(2) • Most projects fail at implementation! • The technology only works if people want it and use it • Requires emphasis on participation, ownership, training, respect for practicalities • ‘Implementation’ begins with design • Evaluation begins with design • Formative evaluation essential • See Shortliffe Shortliffe: The Adolescence of AI in Medicine: Will the Field Come of Age in the 1990's? Artificial Intelligence in Medicine, 5:93-106, 1992. http://smi-web.stanford.edu/pubs/SMI_Abstracts/SMI-92-0449.html www.cs.man.ac.uk/ai/modules/cds
Potted History (1) • Bayesian stream • 1968 Ledley and Lusted: Diagnosis using ‘Idiot Bayes’ discriminant • Followed by Pauker Decision Support using utility theory • 1970-1985 - de Dombal: ‘Idiot Bayes’ abdominal pain and other surgical diagnostic problems • Meanwhile RCP Computer Workshop refined discriminants and then stimulated Spiegelhalter to come up with practical algorithms for belief nets in early 1990s • 1980s Society for Medical Decision Making formed and statistical work largely separated from rule based work www.cs.man.ac.uk/ai/modules/cds
“Idiot Bayes” • A simple statistical means to use databases to determine weights. • Collect a sample of patients with each disease, e.g.Acute Abdominal Pain patients 100 each ofAppendicitis, Cholecystitis, Pancreatitis, Perforated Ulcer, Obstruction, GI Cancer, Tubal pregnancy (in women only) • Add a catch-all for everything else “Non specific Abdominal pain” • Assume that all symptoms are caused independently by each disease –e.g. that the mechanisms for rebound tenderness and nausea are different. • Derive a table of probabilities to be combined using the “Idiot Bayes’ formula • Proved much more robust than less “idiotic” methods www.cs.man.ac.uk/ai/modules/cds
Potted History (2) • Rule based stream • 1972 - Shortliffe Mycin: First rule based system • 1970s US AIM Workshop produced “Big 4” • Mycin/Oncocin/Puff - Backwards chaining ‘shells’ • Interist I - NEJM CPCs from a large network • Became QMR as a general reference • Casnet - Multilayer causal reasoning (glaucoma) • Abel - Complex causal networks (acid-base metabolism) • 1990s Protocol based reasoning • Protégé/Eon successors to Mycin/Oncocin at Stanford • Musen MA. Domain ontologies in software engineering use of Protégé with the EON architecture. SMI Technical Report 97-0657. Methods of Information in Medicine 37:540-550, 1998. • ProForma at ICRF • ASBRU • PRODIGY III www.cs.man.ac.uk/ai/modules/cds
Typical Mycin Rules • IF the gram-stain is gram-negativeAND if the culture-site is sterileAND if the culture-site is bloodAND if the aerobicity is anerobicTHEN there is strong (.8) evidence that the organism is enterobacter • Based on expert opinion rather than data www.cs.man.ac.uk/ai/modules/cds
Potted History (3) • Reminders • 1970 - Homer Warner, HELP, LDS • 1980s - Arden Syntax • 1990s - MLMs - standardised Arden • 1970s - Clem McDonald - ‘…reminders and the nonperfectability of man” • Regenstrief laboratory systems • Many variations • PRODIGY II • Systematic Review: Johnston M, Langton K, Haynes R and Mathieu A (1994). www.cs.man.ac.uk/ai/modules/cds
Potted History (4) • Offshoots and Idiosyncratics • Critiquing - Perry Miller • Also Johan van der Lei • Quick Medical Reference - Chip Masari • Intelligent Records - Alan Rector and Anthony Nowlan • Knowledge Couplers - Larry Weed www.cs.man.ac.uk/ai/modules/cds
Potted History (5) • Knowledge Management and the Web • 1980s Grateful Med and DxPlain • Quick access to Medline abstracts and related • 1990s “The Web with everything” • Rise of Evidence Based Medicine • Cochrane, NICE, NELH, Health on the Web (HoN),… • Indexing and ‘meta data’ • How do you find it • Portals and certification • How do you know if it is any good • Information for Public and Patients • Its an open world out there • Type “Diabetes Support” at Google 776,000 hits, AllTheWeb 295,000Yahoo 26, Netscape 2000 • Classic Information Retrieval and Librarianship • Digital Libraries • Different fields with little contact www.cs.man.ac.uk/ai/modules/cds
Examples of Web Based Initiatives • DxPlain • PaperChase • Health on the Net (HoN) • OpenClinical • Baby CareLink • Guardian Angels • … and of course PubMed and the NLM initiatives www.cs.man.ac.uk/ai/modules/cds
Why isn’t decision support in routine use? • Hypothesis one: “Pearls before swine” • Doctors are ‘resistant’ • Hypothesis two: “The Emporer’s new clothes” • Systems are not clinically worthwhile • Not clinically useful • Too time consuming - too hard to learn • Too expensive • Too inaccessible • Too sparse • How many diabetic patients does a GP see per week? • Easier ways to get help • The technology is still primitive • Developers misunderstand medicine • They think it is rational! www.cs.man.ac.uk/ai/modules/cds
Why isn’t decision support in routine use? • Hypothesis 3: “The invisible computer” • When it works, no one notices • ECG interpretation • Alerts and reminders • NHS Direct • Simple but effective? • Junior doctors’ PDAs • Convergence of communication and computing • Upmarket PDAs have 10-100 times the power of the machine that first ran Mycin! • Why Web technology and XML are critical to this course • divorce content and presentation www.cs.man.ac.uk/ai/modules/cds
What would you want from decision support? • Discussion break www.cs.man.ac.uk/ai/modules/cds
Some Technical Issues • Technical • Re-use, transfer, and Terminology • Links to medical records • Protocols and Problem Solving Methods • Combinatorial explosions • Context and common sense • Cognitive utility • The demise of the ‘oracle’ • The difficulty of ‘mixed initiative systems’ www.cs.man.ac.uk/ai/modules/cds
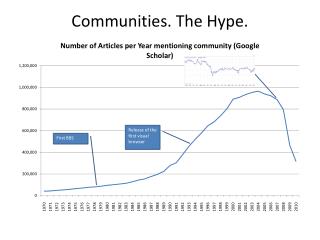
The Interface of Three Technologies /Modelling Paradigms • Terminology and Ontologies • Electronic Patient Records • Decision Support/Inferencing • including ‘abstraction’ • Plus Information Management/Information Retrieval www.cs.man.ac.uk/ai/modules/cds
Patient Specific Records (1) Information Model(Patient Data Model) interface interface Inference Model(Guideline Model) Concept Model(Ontology) interface Dynamic Guideline Knowledge (2b) Static Domain Knowledge (2a)
A Protocol www.cs.man.ac.uk/ai/modules/cds
Who Should Be Evaluated for UTI? Under the assumptions of the analysis, all febrile children between the ages of 2 months and 24 months with no obvious cause of infection should be evaluated for UTI, with the exception of circumcised males older than 12 months. Minimal Test Characteristics of Diagnosis of UTI To be as cost-effective as a culture of a urine specimen obtained by transurethral catheter or suprapubic tap, a test must have a sensitivity of at least 92% and a specificity of at least 99%. With the possible exception of a complete UA performed within 1 hour of urine collection by an on-site laboratory technician, no other test meets these criteria. Performing a dipstick UA and obtaining a urine specimen by catheterization or tap for culture from patients with a positive LE or nitrite test result is nearly as effective and slightly less costly than culturing specimens from all febrile children. Treatment of UTI The data suggest that short-term treatment of UTI should not be for <7 days. The data do not support treatment for >14 days if an appropriate clinical response is observed. There are no data comparing intravenous with oral administration of medications. Evaluation of the Urinary Tract Available data support the imaging evaluation of the urinary tracts of all 2- to 24-month-olds with their first documented UTI. Imaging should include VCUG and renal ultrasonography. The method for documenting the UTI must yield a positive predictive value of at least 49% to justify the evaluation. Culture of a urine specimen obtained by bag does not meet this criterion unless the previous probability of a UTI is >22%. FOOTNOTES The recommendations in this statement do not indicate an exclusive course of treatment or serve as a standard of medical care. Variations, taking into account individual circumstances, may be appropriate. www.cs.man.ac.uk/ai/modules/cds
Semi Structured in GEM as seen in Gem Cutter www.cs.man.ac.uk/ai/modules/cds
Terminology, Medical Records, and “the curly bracket problem” • Re-use • Why should everyone start from scratch? • Attempts to transplant HELP complete did not work • Could we transfer fragments of Help? • Workshop at IBM centre at Arden near New York City produced generalisation of HELP syntax: • The Arden Syntax - now renamed Medical Logic Modules, MLMs www.cs.man.ac.uk/ai/modules/cds
Example Arden Syntax • Data Slot creatinine := read {'dam'="PDQRES2"}; last_creat := read last {select "OBSRV_VALUE" from "LCR" where qualifier in ("CREATININE","QUERY_OBSRV_ALL")}; • Items in curly brackets {…} are institution specific Source: MLM Tutorial AMIA 2001 here www.cs.man.ac.uk/ai/modules/cds
Arden Syntax - Next bit but from another institution data: creatinine_storage := event {'32506','32752'; /* isolated creatinine */ ...'32506','33801'; /* chem 20 */}; evoke: creatinine_storage;; • Items in curly brackets {…} are institution specific www.cs.man.ac.uk/ai/modules/cds
The ‘Curly Bracket Problem’ • Transfering the logic is easy • Transfering the access rules in curly brackets is hard • And it takes your most skilled people • Subtle dependencies and system indiosyncracies • The need for a common vocabulary www.cs.man.ac.uk/ai/modules/cds
Clinical Terminology Data Entry Clinical Record Decision Support Data Entry Decision Support &Aggregated Data GALENClinicalTerminology Electronic Health Records Where we come from Best Practice Best Practice www.cs.man.ac.uk/ai/modules/cds
Controlled Vocabularies and ‘Ontologies’ • A common theme • Affects Protégé/Eon, ProForma, ASBRU etc • Protégé/Eon based on Shared Problem Solving Methods (PSM) and shared Ontology • A library of PSMs. No reused ontologies! • The glue to link Medical Records and Clinical Decision Making • But only half the problem • Systems must have the same concepts • Doctors must use the same concepts • But made worse because most vocabulary is so awful to use www.cs.man.ac.uk/ai/modules/cds
The Link to Medical Records • The Terminology provides the content for the boxes in the information model www.cs.man.ac.uk/ai/modules/cds
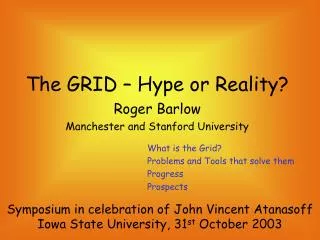
Infection Surgical Procedure Disease has treatment Surgical has diagnosis Patient Disease Procedure has complication www.cs.man.ac.uk/ai/modules/cds
Mrs Smith Infection Surgical Procedure Disease Excision Infection Melanoma has treatment has diagnosis Excision Melanoma has complication www.cs.man.ac.uk/ai/modules/cds
Protocols and Problem Solving Methods • Machines and people • If it is easy for people it is hard to specify logically and program • and vice versa • A real Guideline from NICE here • And from GEM site here • What do you do with one of these? • What does it mean operationally? • See next page for extract from GEM site protocol on UTI in children www.cs.man.ac.uk/ai/modules/cds
How might we do it? • Can you make a simple “Clinical Algorithm” from the previous? • Can you scale this up to a cancer chemotherapy protocol www.cs.man.ac.uk/ai/modules/cds
Today’s Standards • EHRs • HL7 v2 and v3 • OpenEHR / CEN 13606 / Ocean Informatics Archetypes • Terminology • SNOMED-CT • Clinical Terms V2 • ICD 9/10 (CM) • Specialist terminologies www.cs.man.ac.uk/ai/modules/cds
HL7 - A Very Brief Intro www.cs.man.ac.uk/ai/modules/cds
Patient Organization Place ActRelationship confidentialityCode : CE addr : BAG<AD> mobileInd : BL ManagedParticipation typeCode : CS veryImportantPersonCode : CE standardIndustryClassCode : CE addr : AD id : SET<II> inversionInd : BL directionsText : ED outboundRelationship statusCode : SET<CS> contextControlCode : CS Access positionText : ED LicensedEntity 0..n 0..n contextConductionInd : BL approachSiteCode : CD gpsText : ST sequenceNumber : INT recertificationTime : TS Person targetSiteCode : CD 1 1 source priorityNumber : INT gaugeQuantity : PQ addr : BAG<AD> pauseQuantity : PQ Act Participation maritalStatusCode : CE checkpointCode : CS classCode : CS educationLevelCode : CE Entity typeCode : CS splitCode : CS Role moodCode : CS raceCode : SET<CE> classCode : CS functionCode : CD player joinCode : CS id : SET<II> disabilityCode : SET<CE> classCode : CS contextControlCode : CS ... determinerCode : CS negationInd : BL 0..1 0..1 code : CD 0..n 0..n livingArrangementCode : CE id : SET<II> sequenceNumber : INT id : SET<II> 0..n 0..n conjunctionCode : CS 1 1 negationInd : BL religiousAffiliationCode : CE code : CE code : CE playedRole negationInd : BL localVariableName : ST 1 1 derivationExpr : ST ethnicGroupCode : SET<CE> negationInd : BL noteText : ED quantity : SET<PQ> 0..n 0..n seperatableInd : BL text : ED addr : BAG<AD> time : IVL<TS> name : BAG<EN> inboundRelationship 0..n 0..n title : ST telecom : BAG<TEL> desc : ED modeCode : CE statusCode : SET<CS> statusCode : SET<CS> statusCode : SET<CS> awarenessCode : CE target scopedRole LivingSubject effectiveTime : GTS effectiveTime : IVL<TS> signatureCode : CE existenceTime : IVL<TS> ... 0..n 0..n activityTime : GTS 1 1 administrativeGenderCode : CE certificateText : ED telecom : BAG<TEL> signatureText : ED 0..1 0..1 availabilityTime : TS birthTime : TS quantity : RTO source riskCode : CE performInd : BL priorityCode : SET<CE> ControlAct deceasedInd : BL scoper positionNumber : LIST<INT> ... substitutionConditionCode : CE ... handlingCode : CE 1 1 confidentialityCode : SET<CE> ... deceasedTime : TS target 1 1 repeatNumber : IVL<INT> multipleBirthInd : BL 1 1 interruptibleInd : BL multipleBirthOrderNumber : INT WorkingList levelCode : CE organDonorInd : BL Employee 0..n 0..n outboundLink FinancialContract ownershipLevelCode : CE independentInd : BL 0..n 0..n jobCode : CE RoleLink paymentTermsCode : CE uncertaintyCode : CE jobTitleName : SC typeCode : CS Material inboundLink reasonCode : SET<CE> NonPersonLivingSubject jobClassCode : CE effectiveTime : IVL<TS> ... formCode : CE languageCode : CE strainText : ED salaryTypeCode : CE salaryQuantity : MO InvoiceElement genderStatusCode : CE hazardExposureText : ED modifierCode : SET<CE> SubstanceAdministration protectiveEquipmentText : ED ManufacturedMaterial Observation unitQuantity : RTO<PQ,PQ> routeCode : CE 0..n 0..n unitPriceAmt : RTO<MO,PQ> lotNumberText : ST value : ANY approachSiteCode : SET<CD> netAmt : MO LanguageCommunication interpretationCode : SET<CE> expirationTime : IVL<TS> doseQuantity : IVL<PQ> Procedure factorNumber : REAL methodCode : SET<CE> stabilityTime : IVL<TS> languageCode : CE rateQuantity : IVL<PQ> methodCode : SET<CE> pointsNumber : REAL targetSiteCode : SET<CD> modeCode : CE doseCheckQuantity : SET<RTO> approachSiteCode : SET<CD> proficiencyLevelCode : CE maxDoseQuantity : SET<RTO> targetSiteCode : SET<CD> preferenceInd : BL Device DiagnosticImage Account manufacturerModelName : SC softwareName : SC subjectOrientationCode : CE name : ST Container balanceAmt : MO localRemoteControlStateCode : CE ... PatientEncounter capacityQuantity : PQ currencyCode : CE alertLevelCode : CE PublicHealthCase Supply heightQuantity : PQ lastCalibrationTime : TS preAdmitTestInd : BL interestRateQuantity : RTO<MO,PQ> detectionMethodCode : CE quantity : PQ diameterQuantity : PQ admissionReferralSourceCode : CE allowedBalanceQuantity : IVL<MO> transmissionModeCode : CE expectedUseTime : IVL<TS> capTypeCode : CE lengthOfStayQuantity : PQ diseaseImportedCode : CE RIM 2.01 separatorTypeCode : CE dischargeDispositionCode : CE July 17,2003 FinancialTransaction barrierDeltaQuantity : PQ specialCourtesiesCode : SET<CE> Diet DeviceTask bottomDeltaQuantity : PQ specialAccommodationCode : SET<CE> amt : MO energyQuantity : PQ parameterValue : LIST<ANY> acuityLevelCode : CE creditExchangeRateQuantity : REAL carbohydrateQuantity : PQ debitExchangeRateQuantity : REAL HL7 Reference Information Model (The RIM) www.cs.man.ac.uk/ai/modules/cds
ActRelationship typeCode : CS inversionInd : BL outboundRelationship contextControlCode : CS 0..n 0..n contextConductionInd : BL sequenceNumber : INT 1 1 source priorityNumber : INT pauseQuantity : PQ Act Participation checkpointCode : CS classCode : CS Entity typeCode : CS splitCode : CS Role moodCode : CS classCode : CS functionCode : CD player joinCode : CS id : SET<II> classCode : CS contextControlCode : CS ... determinerCode : CS negationInd : BL 0..1 0..1 code : CD 0..n 0..n id : SET<II> sequenceNumber : INT id : SET<II> 0..n 0..n conjunctionCode : CS 1 1 negationInd : BL code : CE code : CE playedRole negationInd : BL localVariableName : ST 1 1 derivationExpr : ST negationInd : BL noteText : ED quantity : SET<PQ> 0..n 0..n seperatableInd : BL text : ED addr : BAG<AD> time : IVL<TS> name : BAG<EN> inboundRelationship 0..n 0..n title : ST telecom : BAG<TEL> desc : ED modeCode : CE statusCode : SET<CS> statusCode : SET<CS> statusCode : SET<CS> awarenessCode : CE target scopedRole effectiveTime : GTS effectiveTime : IVL<TS> signatureCode : CE existenceTime : IVL<TS> ... 0..n 0..n activityTime : GTS 1 1 certificateText : ED telecom : BAG<TEL> signatureText : ED 0..1 0..1 availabilityTime : TS quantity : RTO source riskCode : CE performInd : BL priorityCode : SET<CE> scoper positionNumber : LIST<INT> ... substitutionConditionCode : CE ... handlingCode : CE 1 1 confidentialityCode : SET<CE> target 1 1 repeatNumber : IVL<INT> interruptibleInd : BL levelCode : CE 0..n 0..n outboundLink independentInd : BL 0..n 0..n RoleLink uncertaintyCode : CE typeCode : CS inboundLink reasonCode : SET<CE> effectiveTime : IVL<TS> ... languageCode : CE HL7 RIM Backbone (UML) www.cs.man.ac.uk/ai/modules/cds
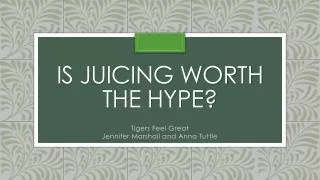
HL7 RIM Backbone as Block-Diagram www.cs.man.ac.uk/ai/modules/cds
HL7 Data in XML <act classCode=“ACT” moodCode=“…”> <id root=“1.3.6.1.4.1.12009.3” extension=“A1234”/> <code code=“...” codeSystem=“2.16.840.1.113883.6.1”/> <participant typeCode=“…”> <participant classCode=“ROL”> <id root=“1.3.6.1.4.1.12009.4” extension=“1234567-8”/> <code code=“…” codeSystem=“2.16.840.1.113883.6.21”/> <playingEntity classCode=“ENT”> <name>...</name> </playingEntity> <scopingEntity classCode=“ENT”> <name>...</name> </scopingEntity> </participant> </participant> <sourceOf typeCode=“REL”> <target classCode=“ACT”> <id root=“1.3.6.1.4.1.12009.3” extension=“A1235”/> </target> </sourceOf> </act> www.cs.man.ac.uk/ai/modules/cds
Refined Model – Observation on Patient www.cs.man.ac.uk/ai/modules/cds
Observation on Patient in XML <observationEvent classCode=“OBS” moodCode=“EVN”> <id root=“1.3.6.1.4.1.12009.3” extension=“A1234”/> <code code=“...” codeSystem=“2.16.840.1.113883.6.1”/> <subject typeCode=“…”> <patient classCode=“ROL”> <id root=“1.3.6.1.4.1.12009.4” extension=“1234567-8”/> <code code=“…” codeSystem=“2.16.840.1.113883.6.21”/> <patientPerson classCode=“PSN”> <name><given>John</given><family>Doe</family></name> </patientPerson> <providerOrganization classCode=“ORG”> <name>St., Josephs Hospital</name> </providerOrganization> </patient> </subject> <component typeCode=“REL”> <observationEvent classCode=“ACT”> <id root=“1.3.6.1.4.1.12009.3” extension=“A1235”/> </observationEvent> </component> </observationEvent> www.cs.man.ac.uk/ai/modules/cds
Refined Model – Observation on Trial Subject www.cs.man.ac.uk/ai/modules/cds
Observation on Trial Subject in XML <observationEvent classCode=“OBS” moodCode=“EVN”> <id root=“1.3.6.1.4.1.12009.3” extension=“A1234”/> <code code=“...” codeSystem=“2.16.840.1.113883.6.1”/> <subject typeCode=“…”> <researchSubject classCode=“ROL”> <id root=“1.3.6.1.4.1.12009.5” extension=“1234567-8”/> <code code=“…” codeSystem=“2.16.840.1.113883.6.21”/> <subjectPerson classCode=“PSN”> <name><given>John</given><family>Doe</family></name> </subjectPerson> <researchSponsor classCode=“ORG”> <name>Eli Lilly</name> </researchSponsor> </researchSubject> </subject> <component typeCode=“REL”> <observationEvent classCode=“ACT”> <id root=“1.3.6.1.4.1.12009.3” extension=“A1235”/> </observationEvent> </component> </observationEvent> www.cs.man.ac.uk/ai/modules/cds
Archetypes • Find on openEHR web site • Google “OpenEHR” www.cs.man.ac.uk/ai/modules/cds
OpenEHR: http://www.openehr.org www.cs.man.ac.uk/ai/modules/cds