Download
1 / 74
740 likes | 742 Views
Learn about common opportunistic infections (OIs) in individuals with HIV, including their manifestations, diagnosis, and treatment options. Discover the typical course of HIV infection and who is most at risk for OIs. Explore examples of common OIs/malignancies, such as Pneumocystis pneumonia and Kaposi's sarcoma.

E N D
Common Opportunistic Infections in HIV infected individuals Ryan Scanlan, PA-C
Opportunistic Infection • “Infection caused by an organism capable of causing disease only in a host whose resistance is lowered (by other diseases or by drugs)”
General Principles • Interaction between virulence of organism and degree of immunodefiency • more virulent organisms can cause disease at higher CD4 counts • Many OIs are reactivations vs. de novo infection • Multiple infections may co-exist • Manifestations of disease may differ in HIV+ patients (vs. HIV -) or among HIV +, based on degree of immunosuppression
Who Still Gets OIs? • Patients not known to have HIV may present with an OI • Patients who are not willing to take or are non-adherent to antiretroviral therapy • Patients with resistant virus who have exhausted available antiretroviral options
Typical Course of HIV Infection Primary Infection 107 1200 Death +/-Acute HIV Syndrome Wide dissemination of virus Seeding of lymphoid organs 1100 1000 Opportunistic diseases 106 Clinical Latency 900 800 105 Constitutional Symptoms 700 600 HIV RNA Copies per ml Plasma 500 104 CD4+ T Lymphocyte Count (cells/mm3) 400 300 103 200 100 0 102 0 3 6 9 12 1 2 3 4 5 6 7 8 9 10 11 Weeks Years Modified from: Fauci AS et al. Ann Intern Med 1996;124-654
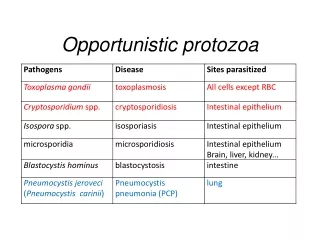
Examples of Common OIs/Malignancies • Pneumocystis carinii (fungus) • Candidiasis (fungus) • Mycobacterium avium complex (bacterium) • Cryptococcal infection • Toxoplasma gondii (parasite) • Cytomegalovirus (virus) • Kaposi’s sarcoma
Pneumocystis jiroveci pneumonia JAMA 2001;286:2450-60
Pneumocystis Pneumonia (PCP) • Caused by pneumocystis jirovecii • Classified as fungus- similar to protozoa • Disease caused by acquisition of new infection, but MOSTLY reactivation of latent infection • Troph vs. cyst
Typical Presentation • Insidious onset of symptoms • Dyspnea on exertion • Nonproductive cough – earlier onset • Fever ~100.5 • Diffuse interstitial infiltrates on CXR (any pattern may be seen, including normal CXR, pneumothoraces) • Tachypnea • Crackles/Rales OR normal lung sounds (50/50)
Differentiation of bacterial pneumonia & pneumocystis pneumonia
Diagnosis of PCP • PulseOx drop on exertion • LDH – also a predictor of mortality • 1-3-beta-d-glucan levels • Sensitivity: • Induced sputum <50-90% • Bronch with BAL 90-99% • TBB 95-100% • Open lung bx 95-100%
Chest CT Normal PCP
Dx requires sputum that shows the organism • Sputum induction with inhaled hypertonic saline • Bronchoalveolar lavage – 3 samples • Immunofluorescent staining using fluorescein-labeled monoclonal antibodies
Treatment of Pneumocystis Pneumonia **Consider adding a corticosteroid
Role of corticosteroids in PCP • Improved short-term mortality and progression to respiratory failure with moderate-severe PCP: either A-a gradient > 35, or pO2 < 70* • Prednisone • 40mg twice daily X 5 days • 40mg daily X 5 days • 20mg daily X 11 days • Adverse events: exacerbation of thrush, herpes (common); also steroid psychosis (rarer) * Gagnon, NEJM 1990
Approach to clinical failure of PCP therapy • Review diagnosis • How was initial dx established? • Was there concurrent process initially? • Has another process supervened? • Immune reconstitution? • Review treatment • Is pt receiving the best PCP treatment? • Is sulfa resistance possible? • Is pt receiving adjuvant steroids? • Is dosing of medication correct? • Does pt have thrush, nausea, emesis, diarrhea? • Adequate time for therapy to work? • Consider further evaluation with bronchoscopy
Drugs for Prophylaxis against Pneumocystis Pneumonia Thomas C and Limper A. N Engl J Med 2004;350:2487
Stopping PCP Prophylaxis • Prophylaxis can be discontinued if plasma HIV-1 viral load undetectable and CD4>200 for at least 3 months • Restart if CD4 decreases <200
Kaposi’s sarcoma • Most common malignancy in AIDS pts – association with cytotoxic T cells • Strong association with Human Herpes Virus-8 • Disproportionately affects gay men – sex, saliva • Patho: Suppression of onco-regulators • Proliferation of abnormal vascular structures – vascular tumor
Kaposi Sarcoma • Skin: painless, firm, slightly raised or nodular tumors – millimeters to centimeters: • Pink to red to purple hue • No discharge, bleeding or necrosis • Lower extremities, face (esp nose), oral muscosa, genitals • Diagnosis requires biopsy – spindle shaped cells with neovascularization of aberrant small vessels that can leak RBCs
Kaposi’s sarcoma • Visceral involvement common -- GI, lungs, oral cavity • Morbidity > mortality • e.g. lymphatic obstruction: edema • Occurs at wide range of CD4 counts, but increased incidence at lower counts • MAY come before cutaneous lesions
Kaposi sarcoma - oral • 1/3 of patients • Pain, bleeding, ulceration - chewing • Secondary infection • Under purview of dental
Kaposi sarcoma – GI tract • 40% at diagnosis, 80% at autopsy –Mouth to anus • Hemorrhagic nodules • weight loss, abdominal pain, nausea and vomiting, upper or lower GI bleeding, malabsorption, intestinal obstruction and/or diarrhea • Again, dx requires bx
Kaposi Sarcoma - lungs • Most common site • lung parenchyma, airways, pleura, and/or intrathoracic lymph nodes • Symptoms contingent upon location – none are distinguishing of KS
Kaposi Sarcoma - lungs • Parenchyma – dry cough, dyspnea, hypoxemia • Airway – intractable cough, hemoptysis, wheezing, obstruction • Pleura - effusion
Kaposi Sarcoma - lungs Plain film – patchy reticular opacities CT – hilar densities/nodules that “fan out” to periphery along perivascular lines
Kaposi Sarcoma - lungs • Bronchoscopy with BAL is the gold standard • Violaceous lesions seen • BAL to r/o infectious etiology • Biopsy NOT recommended
Kaposi Sarcoma - Staging • Cutaneous alone = T0 • CD4>200 = I0 • No constitutional symptoms = S0 • Visceral = T1 • CD4<200 = I1 • Constitutional symptoms present = S1
Kaposi Sarcoma - Treatment • Initiate ART – most lesions regress • Some may require Vinblastine injections directly into lesion sites • If 25+ lesions, symptomatic visceral involvement or IRIS – systemic chemotherapy
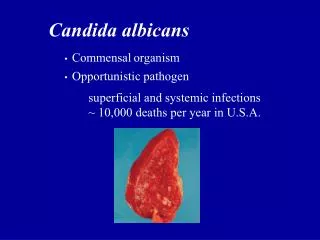
Mucocutaneous candidiasis • Oropharyngeal and esophageal candidiasis • CD4 count most often <200 • Candida albicans in majority • Azole resistance with repeat and long-term exposure • May travel to esophagus
Clinical Manifestations-Oropharyngeal candidiasis • Painless, creamy white, plaque-like lesions on buccal or oropharyngeal mucosa or tongue • Easily scraped off • Less common- erythematous patches on anterior or posterior upper palates or tongue without white plaques • Angular chelitis
Clinical Manifestations-Oropharyngeal candidiasis • Asymptomatic • “Cottony” sensation in mouth • Dysphagia • Loss of taste
Oropharyngeal candidiasis - Diagnosis • Mostly clinic • Scrape and KOH mount – budding yeasts
Oral Candidiasis • Preferred • Fluconazole 100mg/d • Alternative • Nystatin (bitter taste, less effective than clotrimazole) • Clotrimazole troches 10mg 5x/day • Itraconazole swish and swallow liquid • Take on empty sromach • Drug-drug interactions • Ampho B only if failed oral therapy and azole resistance • Treat until sx resolve (usually 10-14 days)
Esophageal Candidiasis • Thrush + odynophagia = presumptive esophageal candidiasis -> Treat • Improvement in 3-4 days • No improvement = endoscopy with biopsy and culture • Preferred tx: Fluconazole(200mg/d po up to 400mg po/d) for 2-3 wks • Alt – Capsofungin or Amphotericin B - toxicities
Esophageal Candidiasis – Maintenance • Consider maintenance in all pts with recurrent esophagitis and low CD4 • Preferred • Fluconazole 100-200mg/d po • Alternative • Itraconazole 200mg/d caps po with food or 100-200mg/d oral solution on empty stomach
Mycobacterium avium complex (MAC) • Includes M. avium and M. intracellulare • Ubiquitous in environment • Pulmonary disease in non-AIDS pts with underlying lung dz and disseminated dz in AIDS • Involves reticuloendothelial system, GI tract • Fever, sweats, wt loss, diarrhea, malaise, anorexia • Anemia
MAC • Occurs at very low CD4 count (< 50) • Diagnosis usually by blood culture Lymph node biopsy
Prophylaxis/Treatment of MAC • Start prophylaxis when CD4 < 50 • Many would obtain baseline AFB blood cx • Can stop when CD4 > 100 x 3 mos • Azithromycin 1200 mg/wk or clarithromycin 500 mg po bid • Treatment: • Clarithromycin 500mg BID+ ethambutol 15mg/kg+/- rifabutin 300mg OD ( adjust if on a PI) • Azithromycin + ethambutol +/- rifabutin • Indefinite tx if CD4 remains low
Most common cause of meningitis in AIDS C. neoformans Reactivation of inhaled microspores CD4 < 100 Fatal within 2 weeks of onset if no treatment started Cryptococcosis
Cryptococcal Meningitis – Clinical Manifestations • Indolent course – low-grade fever, progressive headache, nausea, vomiting. • ¼ with stiff neck – meningeal signs much less common w/ crypto • Photophobia, AMS • Skin – lesions that mimic molluscum contagiosum
Cryptococcal Meningitis = Diagnosis • Clinical Suspicion! • Serum Cryptococcal antigen (CrAg) level – over 99% poz in crypto meningitis • CSF - elevated protein,low WBC and glucose normal or low • Cryptococcal polysaccharide antigen in CSF = treat. • Blood cultures poz in 50-70% • India ink 60-80%
Cryptococcal Meningitis = Diagnosis • Pre-LP – CT of the head for signs of increased ICP and presence of mass lesions • LP – obtain opening pressure (normal below 200 mmH20). • Indicative of increased ICP • Extreme ICP (>350) requires aggressive lowering with repeat LPs, a drain or a shunt • Most common cause of death / Permanent neuro sequela