Download
1 / 40
480 likes | 920 Views
Management of Gastroparesis. Sarah Worah, Dietetic Intern. Sarah Worah Sodexo Dietetic Intern Professional Research Presentation Gastroparesis. WELCOME. Describe signs and symptoms of gastroparesis Identify the Gold Standard for testing and diagnosing gastroparesis

E N D
Management of Gastroparesis Sarah Worah, Dietetic Intern
Sarah Worah • Sodexo Dietetic Intern • Professional Research Presentation • Gastroparesis WELCOME
Describe signs and symptoms of gastroparesis • Identify the Gold Standard for testing and diagnosing gastroparesis • Identify three NUTRITION strategies for managing gastroparesis • Identify current medical management and evaluate their effectiveness OBJECTIVES
Gastroparesis is identified as a syndrome of objectively delayed gastric emptying in the absence of mechanical obstruction and cardinal symptoms including early satiety, postprandial fullness, nausea, vomiting, bloating, and upper abdominal pain (1). Gastroparesis can be caused by neural changes, inflammation, and fibrosis. WHAT IS GASTROPARESIS?
Symptoms are usually similar with different etiologies of gastroparesis (GP) (1) • Nausea • Vomiting • Early satiety • Postprandial fullness • However, in an analysis of 416 patients in the NIH Gastroparesis Registry, patients with idiopathic GP (IG) have more early satiety and abdominal pain compared with patients with diabetic GP (DG) who have more severe retching (1). SYMPTOMS
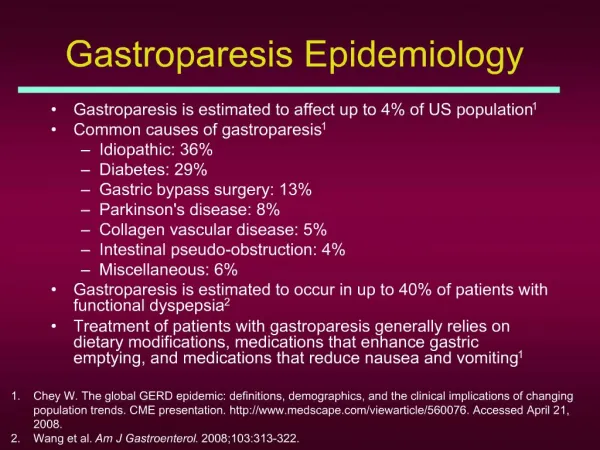
A meta-analysis shows that diabetes is the most commonly recognized systemic disease associated with gastroparesis.Postsurgical (13%), idiopathic (36%) and diabetic etiologies (29%) comprise the majority of cases of GP(1). • More pronounced in DMI (5.2%) than DMII (1%) • Other causes: • Post-viral • Uncontrolled glucose levels • Medication induced CAUSE
Documented delayed gastric emptying is required for the diagnosis of GP (1) • The GOLD STANDARD for testing is the gastric emptying scintography (GES) with solids for 4hr (1, 3) • Shorter tests or tests with liquids can result in decreased sensitivity in the diagnosis of GP (1). • Medications that affect gastric emptying should be stopped 48h before testing • Patients with diabetes should have BG measured before testing- hyperglycemia should be corrected until BG is <275 mg/dL (1). • GP is diagnosed if: • > 90% retention after 1 hour • > 60% retention after 2 hours • >10% retention after 4 hours (3). DIAGNOSIS
ASSESMENT • VITAMIN/MINERAL DEFICIENCIES • ORAL NUTRITION • ORAL SUPPLEMENTS • ENTERAL NUTRITION • PARENTERAL NUTRITION NUTRITION
The primary goal in nutrition support in GP is to prevent or replete fluid, electrolyte, and nutrient deficiencies (1, 2, 3) NUTRITION
Weight loss • < 80% IBW • BMI <20 • Lost 5% of baseline or 5# in 1 month • Lost 10% of baseline or 10# in 6 months (2) • Diet History (3) • 3-5 day food record • Tolerance of types of food • Size/frequency of meals • GI symptoms related to eating • Use of oral supplements • Use of meds affecting GI motility • Laboratory Studies (3) • Ferritin, transferrin, iron • Vitamin B-12, vitamin D, calcium • Glycolatedhemoglobin • Physical (3) • Abd assessment-bowel sounds • General exam for nutrient deficiencies • Hydration status ASSESMENT (1, 2, 3)
The most prevalent vitamin and mineral deficiencies in patient with GP are iron, vitamin D, vitamin B12, and calcium • Two meta-analysis studies recommend (if deficient): • 400-800 IU vitamin D and 1000-1500mg calcium in 500mg doses (2,3) • 150-300 mg elemental iron 3x per day (3) • 350 mcg/day oral B-12, or 1000 mcg intramuscularly 5x days followed by 1000-3000 mcg every 6 months VITAMIN AND MINERAL DEFICIENCIES
Clinical trials examining optimal diet therapy for GP have not been conducted (3) • Recommendations are derived from an empirical approach and physiologic principles (1, 3) ORAL NUTRITION
In a study of 305 patient with GP the average daily caloric intake was 1,168 +/- 801 kcal/day, comprising 58 +/- 39% of daily total energy requirements (3) • Another study reviewed 7-day diet records from 24 symptomatic patients with GP compared with 24 control subjects and found the patients with GP ingested fewer calories than the control group and also were deficient in a number of essential vitamins and minerals (2). ORAL NUTRITION
VOLUME • Small meals is advisable, large meals slow gastric emptying, stomach may empty only 1-2 kcal/min (1,2) • Liquid nutrients should be used d/t gastric emptying of liquids is often normal in patients with delayed emptying of solids (1,2,3) • Oral nutrition supplements • Blenderized solids ORAL NUTRITION
FAT & FIBER • Low-fiber is recommended d/t increased risk for bezoar formation and the decreased ability to clear indigestible fiber from the stomach (2) • Low-fat is sometimes recommended. Fat activates CCK, resulting in fundic relaxation, inhibition of antral motility and delayed gastric emptying. Medium-chain triglycerides do not activate CCK and may be a source of calories (3) • However there is no clinical data to confirm this recommendation. Fat may slow digestion and aggravate symptoms however if the patient tolerates it, let it go, as fat is a significant source of calories (2). ORAL NUTRITION
For patients who are unable to maintain nutrition with oral intake, enteral feeding should be considered (1,2,3). ENTERAL NUTRITION
No trials to compare options for enteral feeding (2) • Success shown with jejunostomy tube, which bypasses the affected stomach (1,3) (post-pyloric) • Refractory nausea and vomiting with recurrent readmission for dehydration a PEG-J may be placed for venting of gastric contents and symptomatic relief as well as medication delivery (3) • Placement of a PEG should be preceded by a successful nasojuejunal feeding (1) • Jejunal feeding maintains nutrition, relieves symptoms, and reduces frequency of hospital admissions for acute exacerbation of symptoms (1). ENTERAL ACCESS
INTUBATIONS FOR DECOMPRESSION AND FEEDING IN PATIENTS WITH GASTROPARESIS
Caloric requirement can be calculated by multiplying 25 kcal by their current body weight in kilograms (1). • For patients that have experienced considerable weight loss, feeding should begin at a reduced calorie level to avoid refeeding syndrome and the significant electrolyte shifts that can occur; watch K+, phos, Mg (1, 2, 3) • Maintain adequate hydration through EN (2, 3) • Once energy goals are met, feeding may be cycled nocturnally over 8-14 hours (3). ENTERAL NUTRITION
A meta-analysis of the treatment of GP show that enteral nutrition should be preferred over parenteral nutrition d/t costs., potential for complications, and ease of delivery (1) • Another shows that intolerance of EN is usually subjective and beliefs about EN lack supporting evidence. EN should be used over TPN (2). • Lastly, a meta-analysis published by Support Line suggests that EN fed patients suffering from refractory nausea and vomiting, repeated episodes of dehydration, difficulty maintaining feeding tube placement, or declining nutritional status should be considered for parenteral nutrition (3). PARENTERAL NUTRITION
Good glycemic control should be the goal • Acute hyperglycemia inhibits gastric emptying, it is assumed that improved glycemic control improves gastric emptying and reduce symptoms (1) BLOOD GLUCOSE CONTROL
RELATIONSHIP OF GLYCEMIC CONTROL AND GASTROINTESTINAL SYMPTOMS OR GASTRIC EMPTYING BLOOD GLUCOSE CONTROL (3)
PHARMACOLOGIC • PROKINETICS • ANTIEMETICS • SURGICAL • BOTOX • GASTRIC PACEMAKER MEDICAL MANAGEMENT
The evidence for the use of prokinetics is based on trials performed two to three decades ago • Current trails being conducted right now are not available but include Gastroparesis Cardinal Symptom Index and the Patient Assessment of Upper Gastrointestinal Disorders- Quality of Life PHARMACOLOGIC
Only US FDA-approved drug for GP • Should be used for no longer than 12-week period • Risk of side effects including tardive dyskinesia REGLAN
Symptoms improved in all 5 studies • Gastric emptying was accelerated • None were conducted for >4 weeks TRIALS OF METOCLOPRAMIDE FOR GASTROPARESIS REGLAN
Similar to Reglan without the neurologic effects (does not cross blood-brain barrier) (3). • Not US FDA approved- available under a special program by the FDA and via other pathways (1). • Main efficacy on nausea and vomiting (1) DOMPERIDONE (NO NOT THE CHAMPAGNE!)
TRIALS OF DOMPERIDONE ON GASTROPARESIS DOMPERIDONE
Meta-analysis shows phenothiazines, antihistamines, serotonin 5-HT3 receptor antagonists, and tricyclic antidepressants can be used for symptomatic relief (3). • Most common: • Compazine • Phenergan • Benadryl • Amitriptyline/nortriptyline • Zofran is used more routinely for chemo and postoperative vomiting and may not have as great of effect on GP. ANTIEMETICS
BOTOX (1) • NOT recommended for patients with GP based on randomized control trials GES: Gastric Electric Stimulation (Pacemaker) (1) • Used in treatment for patients with refractory symptoms. • Symptom severity and gastric emptying have been shown to improve in patient with diabetic GP but not idiopathic or post-surgical GP. SURGICAL
21 year old female DM I (HbA1C 8.2%) 125# UBW Previous fundoplication 1 year prior Presents with refractory nausea and vomiting, pain, uncontrolled blood sugars, dehydration, and weight loss ~now weighs 105#. CASE STUDY
What diagnostic test should be conducted? • What other assessments should be done? CASE STUDY: TESTS
2 hour gastric emptying test shows normal gastric emptying. GP is ruled out and patient is put on narcotics for pain and TPN. What is wrong with this treatment? CASE STUDY
Patient is discharged home and told to increase calories. One month later is back in the ER with nausea/vomiting, dehydration, and weight is now 95#. Celiac and EGD tests come back negative. Now, what treatment should be done? CASE STUDY
Patient is given 4 hour gastric emptying study and shows 47% retention. She is told to follow a low-fat low-fiber diet and sent home. For the next 6 months she is in the ER 2-3 x per month with severe nausea, vomiting, and dehydration. While in the ER she is given Phenergan, Benadryl, and Ativan and the vomiting is stopped. She is sent home on Reglan. However she is unable to take any food by mouth and weight continues to drop. Weight now is 80#. To make situation more complicated- patient is in water skiing accident and breaks both legs. Continues hospital visits multiple times per month. Reglan is stopped d/t neurologic side effects (extreme twitching, stuttering) What is the next step to take with this patent? CASE STUDY
Patient is sent to Kansas City for GES • PEG-J is placed along with pacemaker • MD warns that effects can take up to 6 months • Overnight cyclic EN is started along with high calorie oral nutrition and supplements during the day • Weaned off ALL narcotics • Started on domperidone 40mg/day CASE STUDY
6-months later patient goes back to KC for follow up. Gastric emptying study shows 17% retention after 4 hours and overall symptoms have significantly improved. Weight is stable at 100# and quality of life has improved significantly. PEG is taken out. • 1 year later only 2x hospital visits for GP and weight has remained stable • 2 years later patient trains for ½ ironman and finishes the race with a group of fellow diabetics • 5 years later patient remains stable, finishes school, and enters an internship to become a Registered Dietitian. She still has occasional flare-ups of GP symptoms but is treated in the ER and usually home with in 3-5 days. Regimen: Benadryl/Phenergan/Ativan every 4 hours. Weight 125# HbA1c 7% No hospital visits for 7 months Domperidone 1x per day 30mg + pacemaker + exercise + careful diet CASE STUDY
How have you handled patients you seen in the hospital with GP? • How do these recommendations differ from the way you currently practice? WHAT HAVE YOU SEEN IN YOUR RPACTICE?
Any additional questions/comments? THANK YOU!
Michael Camilleri, M. H. (2013). Clinical Guideline: Management of Gastroparesis. The American Journal of Gastroenterology, 108, 18-37. • Carol Rees Parrish, R. M. (2007). Nutrition Concerns for the Patient with Gastroparesis. Current Gastroenterology Reports, 9, 295-302. • Monica Habib MS, R. L. (2013). Pathophysiology, Diagnosis, and Treatment of Gastroparesis. Support Line, 35 (1), 19-26. • Frank Duffy, R, H. P. McCallum. (2012). Dietary Treatment for Gastroparesis. In, Clinical Gastroenterology: Gastroparesis Pathophysiology, Presentation, and Treatment (pp. 237-256). Springer Science + Business Media, LLC REFERENCES