Download
1 / 19
270 likes | 829 Views
Congenital Vascular Malformations. Chelsey Tinder, MD USF Department of vascular and endovascular surgery. Congenital Vascular Malformations.

E N D
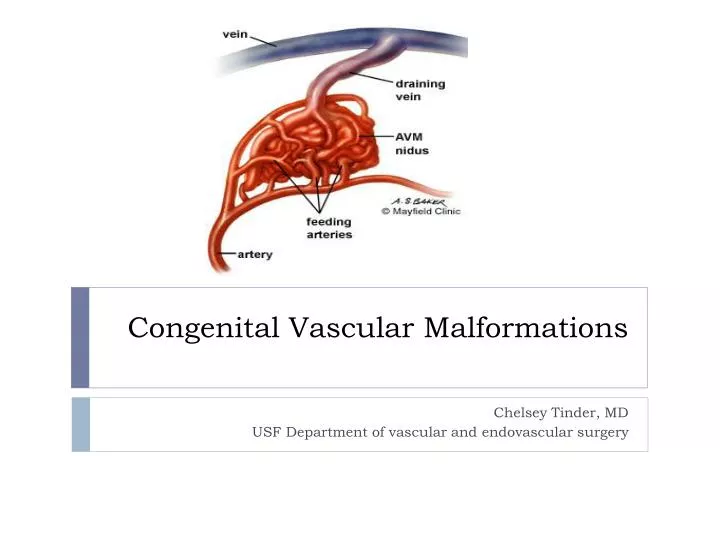
Congenital Vascular Malformations Chelsey Tinder, MD USF Department of vascular and endovascular surgery
Congenital Vascular Malformations • Malformed vessels secondary to arrested development during various stages of embryogenesis, most occur between the 4th and 10th week of embryogenesis • Grow as the child grows, do not regress • Incidence up to 15% of live births • Wide range of presentation with an unpredictable course • 88% asymptomatic • Can involve any organ system, most commonly pelvis, extremities, intracranial circulation
Mulliken Classification • Fast flow lesions • Low flow lesions
Hamburg Classification • Predominately arterial • Truncular • Hypo-, a-, hyperplasia, obstruction, membrane, spur, dilatation • Extratruncular • Infiltrating or limited • Predominately venous • Truncular • Hypo-, a-, hyperplasia, obstruction, membrane, spur, dilatation • Extratruncular • Infiltrating or limited • Predominately AV shunting defects • Truncular • Deep AVF, superficial AVF • Extratruncular • Infiltrating or limited
Hamburg Classification • Combined vascular defects • Truncular • Arterial and venous, hemolymphatic • Extratruncular • Infiltrating hemolymphatic, limited hemolymphatic • Predominately lymphatic defects • Truncular • Hypo-, a-, hyperplasia, obstruction, membrane, spur, dilatation • Extratruncular • Infiltrating or limited
Classification • Extratruncular Lesions • Arrested development early in the embryo • Arise and are composed of mesenchymal cells • Growth influenced by hormones, trauma • Higher rate of recurrence • Compress surrounding structures • Truncular lesions • Occur later in embryogenesis, cells differentiated • More hemodynamically significant
Types of CVM • Capillary malformation • Dilated capillary vessels in the dermis, asymmetric overgrowth of the involved limbs, and sometimes multiple soft tissue tumors • Venous Malformation • Bluish swelling under the skin • Compressible, enlarge with dependence • Increased incidence of thrombosis/PE • Low flow lesions • Lymphatic Malformation • Diffuse (lymphedema) or localized (lymphangioma) swelling
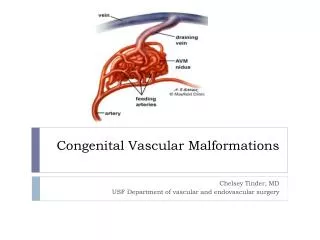
Types of CVM • Arteriovenous malformation • Usually extratruncular • Initially present as local swelling +- thrill, bruits, local hyperthermia • Develop symptoms of shunting – skin necrosis, distal gangrene, high output cardiac failure • Nidus present – central area of AV connection (no capillaries) • High flow lesions • Develop dilated, thickened, tortuous vessels, arterialized veins (medial thickening and fibrosis) • Most morbid, highest rate of recurrence
Noninvasive imaging • MRI • Duplex • Air plethysysmography • Volumetry • Whole-body blood pool scintigraphy • Uses tagged RBCs to detect abnormal blood collections • Radioisotope lymphoscintigraphy • Transarterial lung perfusion scintigraphy • Uses albumin to calculate shunting percentage • CT
Invasive imaging • Angiography • Venography • Lymphangiography
Indications for therapy • Absolute • Hemorrhage • High output cardiac failure • Ischemia • Chronic venous hypertension • Threat to life or vital function • Relative • Disabling pain • Functional impairment • Cosmetically severe deformity • Vascular – bone syndrome • High risk of complications • Lymph leak
Therapy • High flow lesions – Endovascular therapy • Direct puncture, transarterial, or transvenous approach • Superselective catheterization of feeding vessels until identification of nidus • Embolization with polymerizing agents, ethanol (toxic,) detachable balloons, coils can be used definitively • Nitinol mesh plug successful with large AVMs • Temporary occlusion with foams or collagen can be used for preoperative devascularization • Complications include end organ ischemia, embolization, tissue destruction by ethanol, severe swelling with progression to compartment syndrome, PE, arterial emboli, MI from ethanol
Therapy • High flow lesions - open surgical therapy • Often not possible or horribly morbid operations due to complexity and location of lesions • Most suitable for well circumscribed lesions affecting the • Should involve ligation of all feeding vessels and entire malformation unless doing so would result in end organ ischemia, the only potential for cure is complete eradication of the nidus • Incomplete resection can lead to recurrence or block access from an endovascular approach
Therapy • Low flow lesions • Sclerotherapy with ethanol (toxic,) sodium tetradecyl sulfate, polidocanol, ethanolamine oleate, or foam sclerotherapy • Induces direct damage to endothelium resulting in fibrosis and thrombosis • Large lesions require multiple treatments • Complications include tissue destruction by ethanol, nerve damage from slerosing agents, severe swelling with progression to compartment syndrome
Congenital Vascular Malformations • Complex problem with a wide array of manifestations • Therapy often ineffective or palliative, many interventions may be required - complete lesion eradication in only 15% of patients