Download
1 / 58
580 likes | 849 Views
URINARY CATHETER AND GASTRO-INTESTINAL TUBE CARE JANET BOTHA. BY: JANET BOTHA H/N HHCS TABUK. URINARY CATHETER and GASTRO-INTESTINAL TUBE CARE. OBJECTIVES. Encourage all health care workers to avoid urinary catheterization unless clinically indicated

E N D
URINARY CATHETER AND GASTRO-INTESTINAL TUBE CARE JANET BOTHA BY: JANET BOTHA H/N HHCS TABUK URINARY CATHETER and GASTRO-INTESTINAL TUBE CARE
OBJECTIVES • Encourage all health care workers to avoid urinary catheterization unless clinically indicated • Ensure the benefits outweigh the disadvantages and INFORMED consent is obtained • Encourage health education to avoid complications
TOPICS • CONSIDERATIONS AND CLINICAL INDICATIONS • RISK ASSESSMENT • EDUCATION AND CONSENT • CATHETER CARE AND PREVENTION OF INFECTION • OBSERVATION • DOCUMENTATION
CONSIDERATIONS • Must benefit the patient NOT for the convenience of the caregiver • Complications • Informed consent • Patient cognitive status and agitated patient • Time frame of catheterization
CLINICAL INDICATIONS • Acute urinary retention • Bladder irrigation or instillation of medication • Monitoring renal function during critical illness • For a variety of reasons pre-and post operatively • Pressure Ulcers – delayed healing
4 degree Pressure ulcer Healed Ulcer
RISK ASSESSMENT AND POSSIBLE COMPLICATIONS • Allergy • Infection • Trauma • Recent UT surgery • Medication • Obstruction • Pain, discomfort and emotional wellbeing • Diabetes or Chemotherapy • Patient with only one functional kidney or CKD
POSSIBLE COMPLICATIONS • UTI • Serious complications: • pyelonephrites, bacteremia, bladder cancer • Chronic obstruction due to urinary calculi and in male patients, epididymites • Drug resistance due to chronic use of anti-biotics • Urethral necrosis or pressure ulcers
CONSENT • Verbal, written and demonstrative education on total care, regardless of type of catheterization • Informed consent • Risks involved – advantages, disadvantages, complications, and expected timeframe
EDUCTION • Total care • Infection prevention • Obtaining of materials • Care and storage • ID any possible problems –S&S • Where and when to get help by giving contact numbers
SUPRAPUBIC CATHETER • No risk of urethral trauma or necrosis • Greater comfort • Patient can remain sexually active • Micturition still possible
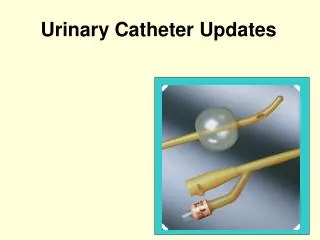
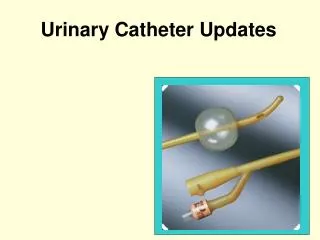
INSERTION OF SUPRA PUBIC CATHETER -Insertion can be done under general or local anesthesia. -A small incision or puncture is made above the pubis and the catheter is inserted. -It could be temporarily or permanent – needs to be changed at 6-12 week intervals.
Supra-pubic catheter
INTERMITTEND SELF-CATHETERIZATION • Reduced infection rate compare to indwelling catheters • Good cognitive ability • Self motivated • Less restriction to movement • Socially more accepted • No visible devices to carry
PROCEDURE • Patient is educated : • Verbal and by demonstration • Correct aseptic technique • Cleansing and storage if the catheter is not disposable • to perform this procedure at 4 hourly intervals • Where to obtain the supplies
Intermittent Self catheterization
INDWELLING CATHETER LONG AND SHORT TERM • Possibility of urethral trauma • Increased risk of infection • Patient needs to carry collection bag • Can impede on emotional wellbeing • Can aid in pressure ulcer healing
PROCEDURE • Use STERILE materials for insertion • Sterile catheter – correct size • Sterile catheter tray • Sterile urine collection bag • Use aseptic technique for inserting catheter • Hand wash • Gown and gloves • Collection bag must be positioned lower than the patient bladder
INFECTION PREVENTION GUIDELINES • Hand washing before and after • Aseptic technique with sterile material when inserting a catheter • Change/removal of catheter at given date • Changing collection bag every 3 days • Good personal hygiene • Adopting closed method of urinary drainage
INFECTION PREVENTION GUIDELINES • Maintaining an aseptic technique when bladder irrigation, medication instillation or collecting of a urine sample is done • Ensuring unobstructed urine flow • Emptying collection bag when it is 1/3 full • Correct positioning of urine collection bag • Traction free urinary catheter • Meatal care • Adequate fluid intake
OBSERVATIONS • Patient health status • Affectivity of antibiotics used • Allergy and tolerance of urinary catheter • Renal status • Ensure that urine flows from catheter into collection bag
OBSERVATIONS • Urine bypassing the catheter • Trauma • Heamaturia, bleeding of the meatus • Erosion, swelling, discharge • Color, odor and volume of urine
DOCUMENTATION • Physicians Order • Indication, type, and brand of catheter • Informed consent • Cognitive state of patient • Date inserted, removal/change • Problems during insertion • Procedures: specimen, irrigation, medication • Fixation • Volume, color, and odor • Education
Gastro-Intestinal Tube Care
GASTRO-INTESTINAL TUBE CARE(naso-gastric tube for feeding) • INDICATION • ADVANTAGES • CONSIDERATIONS • COMPLICATIONS • RISK REDUCTION • MEDICATION ADMINISTRATION • EDUCATION AND MANAGEMENT • DOCUMENTATION
GASTRO-INTESTINAL TUBE CARE(NASO-GASTRIC TUBE for feeding) • INDICATIONS • Blockage in the esophagus • Problems swallowing Tube feedings are given when oral intake is inadequate or not possible and the GI tract is functioning normally. (This procedure is a short term solution to ensure complete nutrition and hydration)
ADVANTAGES • To preserve GI integrity by delivery of nutrients, fluids and medications • To preserve the normal sequence of intestinal and hepatic metabolism • To maintain fat metabolism and lipoprotein synthesis • To maintain normal insulin/glucagon rations • To maintain normal hydration
CONSIDERATIONS • Patient nutritional and hydration status • Is the digestive tract and kidneys functioning • Patient dietary and fluid needs (30-40ml/kg body mass) • Metabolic disorders • Medication in use
CONSIDERATIONS • Informed consent • Responsible caregiver • Cognitive status of patient – restraint • Age and duration • Patient environment
NUTRITIONAL REQUIREMENTS • NUTRIENTS INCLUDES: • Protein • Fat Carbohydrates • Vitamins • Minerals • Fiber
COMPLICATIONS • Aspiration Pneumonia • Accidental dislodging of feeding tube • Difficulty in inserting the tube – epistaxis • Herniation of esophageal varices • Regurgitation and aspiration • nausea
COMPLICATIONS • Pressure ulcer formation • Constipation or diarrhea • Dehydration or over-hydration • Difficulty in cleaning the nasal cavity • Pain and discomfort • Hyperglycemia
INSERTION • Use correct size tube • Measure - tip of nose to earlobe and from earlobe to xiphi sternum and mark the tube • Ensure the nasal cavity is clean • Position the patient • Lubricate the tube • Insert and check position • Fix to nose or convenient area
RISK REDUCTION • ASPIRATION PNEUMONIA • Checking NGT is in correct position before any fluid is given • Correct placement of feed • Proper positioning of patient • (semi-fowlers with head elevated at least 30-45 degrees) • Maintaining this position for at least one hour after the feed • Monitor residual volumes before every feed • If aspiration is suspected, stop feed immediately and suction patient in R lateral position
RISK REDUCTION • DEHYDRATION • Monitor hydration carefully ( patient can in most situation not verbalize thirst) • Water should be given between feeds • Checking of mucous membranes, decreased urine output • Monitor intake and output
RISK REDUCTION • BLOCKING OF TUBE • Tube must be flushed with warm water after every feed • Medication must be crushed into powder form and dissolved in warm water and tube flushed thereafter • Water to be given between feeds • Change tube
MEDICATION ADMINISTRATION • Use medication in liquid form where possible • Ensure whether medication should be given before or after meals • Simple compressed tablets – crush and dissolve in water • Buccal or sublingual tablets must be given as prescribed • Soft gelatin capsules filled with liquid – cut opening and squeeze out contents
MEDICATION ADMINISTRATION • Enteric-coated tablets – do not crush, change in form is required • Timed-release tablets – do not crush, check with pharmacist for alternative • Timed-release capsules or sustained-release capsules – some can be opened and contents added to water – but only after pharmacist was consulted • NEVER mix medication with feed
EDUCATION AND MANAGEMENT All members of the clinical team is responsible to decide if a NGT is appropriate for the patient – Physician, Nurse, Dietician, Pharmacist, Speech Therapist. Education given to the caregiver must be complete and be done verbally and by demonstration to ensure the caregiver is comfortable with the patient and the feeding regime, and know to check if NGT is intact.