Download
1 / 34
340 likes | 569 Views
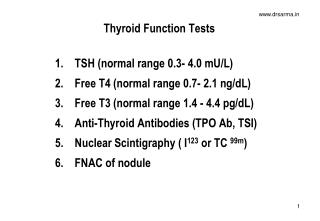
D- Interpreting Thyroid Function Tests. Pt Info: CC: palpitations 82 y/o F presents with hyperactivity, sweating, palpitations, wt loss, insomnia, moist skin, fine hair, irregular menses, diarrhea PE: tachy, elevated SBP, damp skin, lid lag, hyperreflexive DTR

E N D
Pt Info: • CC: palpitations • 82 y/o F presents with hyperactivity, sweating, palpitations, wt loss, insomnia, moist skin, fine hair, irregular menses, diarrhea • PE: tachy, elevated SBP, damp skin, lid lag, hyperreflexive DTR • Labs: CBC wnl, BMP wnl, TSH <0.01 (L), T4 4.1 (H), T3 wnl
Objectives • Pathophysiology • Thyrotoxicosis • Hypothyroid
Hormone Regulation • TRH à TSH • iodine uptake, organification • synthesis & release of thyroid hormone • T4/T3 Regulate: • basal metabolism, thermogenesis, lipogenesis • fetal CNS development
Thyroid Hormones • Triiodothyronine (T3) • 80% in Periphery • Liver/kidney remove iodine from T4 • Regulate Thyroid Hormone-dependent genes • t1/2: 1-1.5 days • Thyroxine (T4) • Thyroid gland • t1/2: 8 days • T4 à T3 • Decreased: • Meds: propranolol, PTU, corticosteroids, amiodarone • Illness: cytokine mediated
Binding Proteins • T4/T3 99% protein bound • Prevents excess tissue uptake • Maintains accessible reserve • Thyroxine-binding globulin (TBG) - 70% • Inc: E2, 5-FU, Methadone, Tamoxifen • Dec: Androgens, Corticosteroids, Niacin • Albumin – 15-20% • Transthyretin – 10-15%
LOW = Hyper Check free T3/T4 NL = No further Testing HIGH = Hypo Check free T4 TSH TFTs
Grave’s Disease • Toxic Adenoma • Toxic Multinodular Goiter • Thyroiditis • Exogenous • TSH Mediated FunctionalDisorders • Hashimoto’s Disease • Post-op/Post-ablative • I deficiency Hypothyroidism Thyrotoxicosis
Thyrotoxicosis • Thyroid excess from any cause: • Increased Synthesis • Damaged Gland • Exogenous Intake • RAIU • High (>30%): Hyperfunction • NL (10-30%): Euthyroid • Low (<10%): Thyroiditis, I excess, Amiodarone
Symptoms • Other: • Pregnancy-related problems • Arthralgias • Skin: hives, itching, vitiligo • Hair loss • Finger/nail changes • Eye: bulging, dry, pain • Depression, irrational anger Increased Metabolism: • Weight loss, Dec appetite • Warm, sweating, thirst, fever • Tachycardia, Arrhythmia, Palpitations • Diarrhea • Fatigue, Exhaustion • Goiter • Difficulty concentrating • Panic and anxiety • Hyperreflexia, Tremors • Insomnia
Thyrotoxicosis • Increased Synthesis • Damaged Gland • Exogenous Intake
Increased Synthesis: Hyperthyroidism • High T4 & Low TSH • Increased T4/T3 release: • Grave’s • Toxic MNG • Toxic Adenoma • High RAIU
Grave’s Disease • Most common cause in US • AutoAb against TSH receptor • Diffuse Goiter, Thyrotoxicosis, High RAIU • Thyroid Scan: Increased activity • Ophthalmopathy, Dermopathy, Acropathy
Grave’s Disease - treatment • Medication: 50% remission @ 1 year • Methimazole • PTU • BB while toxic • Radioactive Iodine Ablation • Not for pts with severe ophthalmopathy • Surgical Removal
Toxic Multinodular Goiter • Sporadic Goiter à Multinodular Euthyroid à Subclinical à Overt Thyrotoxicosis • Increased RAIU (autonomous production) • Rest of Gland suppressed • Treatment: Radioactive Iodine
Toxic Adenoma • HOT Nodule: Autonomous function • Activating Mutation of TSH Receptor • Size = Hormone production • >3 cm • Treatment: • Hemithyroidectomy • Radioactive Iodine
Thyrotoxicosis • Increased Synthesis • Damaged Gland • Exogenous Intake
Damaged Gland • Low RAIU • Subacute Thyroiditis: BB & NSAIDs • Firm & painful gland • Post-viral • Drug-Induced • Amiodarone, Lithium, α-IFN, IL-2 • Postpartum Thyroiditis
Amiodarone-Induced • 3% of patients in US • Type 1: high iodine content (JodBasedow) • Pre-existing thyroid autonomy • High RAIU • Treatment: methimazole • Type 2: direct toxic effect • No Pre-existing thyroid autonomy • Low RAIU, Inc Inflammation • Treatment: Prednisone, NSAIDs
Thyrotoxicosis • Increased Synthesis • Damaged Gland • Exogenous Intake
Surreptitious Intake • Low TSH • Low RAIU • Low TG level
Thyroid Storm • Iatrogenic • Radioiodine therapy, Contrast dyes • Abrupt cessation of Antithyroid drugs • Surgery • Acute Nonthyroidal Illness • Stroke, PE, DKA, Trauma, Infection
Subclinical Thyrotoxicosis • Low TSH & High NL T4 • Complications • Arrhythmia, Osteoporosis • esp >65y/o with TSH <0.1 mU/L
Grave’s Disease • Toxic Adenoma • Toxic Multinodular Goiter • Thyroiditis • Exogenous • TSH Mediated FunctionalDisorders • Hashimoto’s Disease • Post-op/Post-ablative • I deficiency Hypothyroidism Thyrotoxicosis
Hypothyroidism • Low T4 & High TSH • More common than Thyrotoxicosis • Treatment: Synthroid - goal TSH 1-2 mU/L
Symptoms • Accumulation of Matrix Substance: • Skin: coarse/dry, scaly • Hair: coarse/dry, brittle, loss • Hoarseness • Edema of eyes and face • Other: • Arthralgias • Irregular menstrual cycles • Depression Slow Metabolism: • Weight Gain • Constipation • Hypothermia/Cold Intolerance • Fatigued, Lethargy • Slow Movements/speech • Delayed DTRs • Bradycardia
HIGH = Not Enough INC Dose LOW = Too Much DEC Dose NL = Continue Dose TSH Monitoring Replacement
Medication Controversy • ? Generic Synthroid • Not all bioequivalent when FDA approved • ? T3 • 1999: improved mood & psych testing with combo therapy • Four subsequent studies refuted
Hashimoto’s • Most common cause in North America • Positive anti-TPO Ab • Increase Autoimmune Endocrinopathy • Addison’s, DM1, Premature ovarian failure • No further w/u
Myxedema Coma • Obtundation, Hypothermia • CV Changes: • Dec HR, Contractility, SBP, CO • Inc SVR, DBP • Pericardial Effusion • Precipitant: Infection, trauma, cold, sedative
Myxedema Coma - treatment • IV Levothroxine replacement • Corticosteroids – adrenal insufficiency • MV – CO2 retention, hypoxia • Treat precipitating cause
Subclinical Hypothyroidism • High TSH & Low NL T4 • Most have Hashimoto’s • Systemic symptoms, elevated LDL, Cardiac changes
Objectives • Pathophysiology • Thyrotoxicosis • Hypothyroid