Download
1 / 28
280 likes | 516 Views
Urinary Catheterisation and The Law. Karen Ayers RN, BSc Hons Nurse Specialist Continence Care Bradford and Airedale teaching PCT. Objectives. Legal issues with catheterisation Accountability Consent Roles and responsibilities Clinical Governance Documentation Vicarious liability.

E N D
Urinary Catheterisation and The Law Karen Ayers RN, BSc Hons Nurse Specialist Continence Care Bradford and Airedale teaching PCT
Objectives Legal issues with catheterisation Accountability Consent Roles and responsibilities Clinical Governance Documentation Vicarious liability
Skills for Health CC02 You need to apply: Legislation, policy and good practice K1. a working knowledge of the current European and National legislation, national guidelines, organisational policies and protocols in accordance with clinical/corporate governance which affect your work practice in relation to inserting and securing urethral catheters K2. a working knowledge of the importance of working within your sphere of competence and when to seek advice if faced with situations outside of your sphere of competence K3. a working knowledge of the importance of documentation, the data protection act, care of records and disclosure of information with consent from the individual and your employer and the legal and professional consequences of poor practice
What the law says Nurses and support workers have a duty of care to patients. Inexperience is no defence to a claim of negligence. When things go wrong, you are judged against the standard that would reasonably be expected from an ordinarily competent practitioner. There is no excuse for getting basics wrong, such as poor handwriting in a patient record or failing to read relevant patient notes. Employers must ensure staff are trained and supervised to provide care to a legal standard.
Accountability Public - through criminal law Employer - Contract of Employment Patient - Civil Law, duty of care, Common law of negligence Qualified Nurses - NMC Code of Conduct
Delegation Qualified Nurses are professionally accountable for any duties delegated to the HCSW It is crucial that HCSW is appropriately supervised and competent to carry out the task. HCSW must have written evidence of competence in catheterisation from Employer HCSW must recognise any limitations when considering to undertake a delegated catheter change
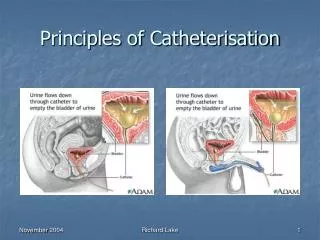
Consent Nurses are accountable for ensuring that patients have given consent for any treatment they are going to receive. Catheterisation without clinical justification and consent can represent assault, battery and /or negligence
12 key points on consent: the law in England (Dh 2001) Before you examine, treat or care for competent adult patients you must obtain their consent Adults are assumed to be competent unless demonstrated otherwise Patients may be competent to make some health care decisions even if not competent to make others Giving and obtaining consent is not usually a one – off event, it is a process. You should always check before caring / treating a patient.
Children aged 16 and 17 are presumed to be competent to consent. Younger children who fully understand can also consent. • The person treating the patient should seek consent from the patient. • Sufficient information should be given i.e. benefits and risks, and alternative treatments. If inadequate information is given the consent may not be valid • Consent must be given voluntarily, not under duress from health professionals, family of friends • Consent can be written, oral or non verbal. A signature does not prove the consent to be valid
Competent adults are entitled to refuse treatment, even when it would clearly benefit their health. Only exception is in case of patients detained under the mental health act with a mental disorder. • No – one can give consent on behalf of an incompetent adult. However treatment can be given if it is in the patients best interests. • If an incompetent patient has indicated in the past, while competent that they would refuse treatment in certain circumstances (an “advance refusal”) this must be adhered to. • More detail can be found in the DH publication “Reference guide to consent for examination or treatment” www.doh.gov.uk/consent
What does consent really mean if you are a patient? You have a choice You must have enough information to enable you to make a decision You can say no or ask for more information You must be acting under your own free will You must be able to give your consent Consent – what you have a right to expect A guide for adults, DH 2001
What is Vicarious Liability? The employing organisation is liable for “systematic errors”, e.g. fault in the system, or inadequate staff training If employee acting in connection with employment when patient harmed, employer is vicariously liable for the employees actions This needs to be understood by employers when inviting staff to change their roles Onus is on the employer to ensure staff adequately trained
Patient Education Procedure explained Catheter care education Patient / Carer able to care for catheter Hygiene / hand washing Avoiding Constipation Signs of complications -blockage, UTI.
Product Liability Catheters and drainage equipment must be used as instructed by manufacturers, otherwise the nurse may be liable. Manufacturers are required to ensure that products conform to British Standards 1695 (1990) Check packaging and expiry date Store according to manufacturers instructions
Principles of Documentation The law assumes that if the work was not documented it was not done. Frank-Stromborg and Christensen 2001; NMC 2005
Nursing records -A legal document Society is becoming more litigious Patients are encouraged to complain about the care they receive Any court can request nursing documentation be presented to a court of law. Analysis of nursing records demonstrates if the Nurse has understood and honoured their duty of care (RCN 2003, NMC 2005)
NMC Guidance for Record Keeping Be factual, consistent and accurate Document soon after an event has occurred Write clearly. Alterations to be dated, timed and signed so original entry can be read clearly Be accurately dated, timed, signed with signature printed on first entry Not include abbreviations, jargon, meaningless phrases, irrelevant speculation and offensive subjective statements Be readable on any photocopier
Documentation Reason for catheterisation Date and time insertion Type of catheter- ch, length, material, balloon size, batch no, manufacturer Cleansing solution, lubricant, anaesthetic agents Any problems encountered Date for reassessment, planned change Signature
So what can go wrong? False passage Bleeding Urethral trauma UTI Septicaemia Death
Nurse Gets Struck Off For Cruelty A former nurse at a Nursing Home in Bradpole has been struck off the nursing register for her conduct including bending a 97-year-old lady's leg, until it cracked, whilst inserting a catheter. The former nurse did not attend the hearing saying that she had retired from nursing for personal reasons.
A 75 year old lady with advanced dementia was admitted to an acute medical ward following a collapse. • Her daughter, a Nurse was horrified when she noticed that her mother had been catheterised for no apparent reason other than management of incontinence. • After discussion with the staff the catheter was removed. • Symptoms of a UTI were observed the following day. • Antibiotic therapy was commenced. • However the lady died 7 days later. • The cause of death? • Septicaemia secondary to UTI
Questions to be asked about this case Why was the catheter put in? Whose decision was it? Was it in the patients best interests? How was informed consent obtained?
Case scenario for discussion You are asked to visit an elderly gentleman to replace his long term indwelling catheter. The qualified Nurse has prescribed catheters and asks you to take them to the house. The catheterisation is uncomplicated and you leave the patient comfortable. 7 weeks later it comes to light that the you inserted a short term catheter (14 days). Who is to blame for this error : You, the qualified Nurse or both of you?
So ….in a nutshell, you should Always act in the patients best interest Recognise your own limitations Regularly update your knowledge Adhere to local policy Always obtain informed consent Use catheter equipment appropriately Report any concerns to a qualified Nurse Document the necessary details correctly Don’t be afraid to challenge practice if you are in doubt