Download
1 / 44
440 likes | 542 Views
Assessing Aphasia and Neurogenic CDs. Localizationists. Franz Gall (early 1800s) Paul Broca (1850s): a neurologist----“articulate speech” located in the posterior-inferior frontal lobe

E N D
Localizationists • Franz Gall (early 1800s) • Paul Broca (1850s): a neurologist----“articulate speech” located in the posterior-inferior frontal lobe • Karl Wernicke (1874): a German neuropsychiatrist published work on “sensory aphasia” –lesions in the posterior temporal lobe
Anti-localizationists • Marie Jean-Pierre Florens (colleague of Gall!) was the first • John Hughlings Jackson (NHNSND) a British neurologist—early 1900s • Henry Head—British neurologist---1920s • Equipotentialists • Lead to theories of cerebral dominance
Language and Cerebral Dominance • Left hemisphere dominance for sph/lang was Broca---early thoughts were that left and right halves of the brain were mirror images on one another • Symmetry notion lasted until Goodglass and Kaplan, Penfield and Roberts (1950s)!! • Confusion about function: right handed people were left hemisphere dominant
Therefore, • Left handed people must be right hemisphere dominant????? • Only a theory based upon case studies • Maybe from an effort to “equalize” theories---make things “symmetrical” • Think of theories of phonation---honest! • (neurochronaxic theory!)
50s researchers noticed • Both left and right handed people had similar problems after brain injury • We learned from the early sodium amytal studies that a small # of people are right hemisphere dominant • Most adults are left hemisphere dominant for sph/language • The question is: how are we born? • Think cerebral plasticity……
Implications of cerebral plasticity • Younger injuries have greater opportunity to improve • Older patients recover less language function than younger patients • The older the patient at the time of injury the more severe the persistent consequences of the injury
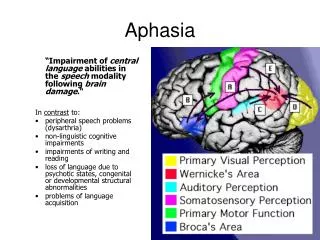
Connectionists These theories focus on function of areas surrounding the injury; in the case of language impairment • The periSylvian region of the left frontal lobe is sometimes called the anterior language zone • Important for planning and executing language: speech, writing, and maybe gestures • The periSylvian region in the left temporal lobes is the posterior language zone • For comprehending and formulating linguistic messages with accurate syntax and semantic structures
Anterior Language Zone • Posterior frontal lobe, just anterior to the motor strip • Holds the location of Broca’s area: the motor speech planning site • Broca’s area: responsible for planning & organizing speech movements for the primary motor cortex • Injury here produces Broca’s aphasia
Posterior Language Zone • Located in the posterior superior left temporal lobe • a.k.a. Wernicke’s area • Sometimes called the auditory association cortex • Important for storage and retrieval of mental representations for words, word meanings, grammatical and linguistic rules
Remember the connectionists? • Wernicke’s gets most of its input from the primary auditory cortex (Heschl’s Gyrus) • Function of the primary auditory cortex is perception and discrimination of auditory stimuli • If a tree falls in the woods and there is no one there to hear it……….
More connectionists • Wernicke’s and Broca’s are connected by a large bundle of nerve fibers (a fasciculus) • Runs between the mid temporal lobe and the frontal lobe via the parietal lobe • The arcuate fasciculus is the primary route by which linguistic messages formulated in Wernicke’s are transmitted forward to Broca’s area
The angular gyrus • At the junction of the temporal, parietal and occipital lobes • Important for processes in reading and writing • Damage to the angular gyrus causes: • Alexia: reading impairment • Agraphia: writing impairment
Language Functions • Comprehension of speech • Spontaneous speech • Repetition • Oral Reading • Writing • Gestural responses to spoken commands
“Fluency” • Important to understanding the connectionist model because connectionist aphasia syndromes are divided into “fluent” and “non-fluent” types. • Relationship between: speech fluency, paraphasia, repetition and language comprehension.
Fluent (aphasic patients) have normal or near normal speech rates and use a variety of different grammatical constructions; function words and grammatical inflections are present, and usually syntactically appropriate. Intonation patterns are present and usually appropriate. Nonfluent (aphasic patients) have slow and labored speech. The variety of grammatical constructions is often restricted and intonation may be reduced or absent; function words and grammatical affixes may be omitted, and patients may rely a lot on nouns (Howard & Hatfield, 1987, p. 147).
Fluent Damage posterior to the Rolandic Fissure Sph flows smoothly and effortlessly Fluent aphasic spkrs. Usually manipulate rate, intonation, and stress Non Fluent Damage anterior to the Rolandic Fissure Sph is halting and made with great effort Rate is slower than normal, intonation is limited, stress is missing (diminished) Connectionist Aphasia Syndromes
Paraphasias • “errors in speaking produced by speakers with aphasia” (Brookshire) • 2 forms: literal and verbal paraphasia • Literal paraphasia: phonologic (phonemic) errors----”tootbrust” for toothbrush • Verbal paraphasia: semantic errors (usually related to the term) as in “knife” for fork • Sports talk: “play was admiral; defense had pronouns” • NOTE: literal paraphasia vs. apraxia
Repetition • Variations in speech repetition and language comprehension are indicators of several fluent aphasia “syndromes”
Classical Aphasia Syndromes • Broca’s aphasia** • Wernicke’s aphasia** • Global aphasia** • Conduction aphasia • Transcortical motor aphasia • Transcortical sensory aphasia • Mixed aphasia • Disconnection syndromes
Broca’s aphasia • Expressive, motor or anterior aphasia • Because of proximity to the motor strip (face, hand and arm) and because descending pyramidal fiber tracts run alongside Broca’s area: pts with Broca’s display right-sided hemiplegia or hemiparesis
Broca’s area • Lower part of the premotor cortex; just anterior to the primary motor cortex • Premotor cortex: plans skilled voluntary movements for the motor cortex in both hemispheres • Broca’s area is adjacent to motor cortex of the face; thus it is the speech motor planner
Speech style • Slower rate, laborious movement, halting • Long pauses between words; sometimes even within words • Lacking intonation • Misarticulations are common; some consonants and vowels are distorted • Short phrases usually missing functor words I.e., conjunctions, prepositions and articles
Speech style: Broca’s • Missing functor words causes the description of agrammatic; sometimes called telegraphic • Next slide is from from a patient describing a picture from the Boston Diagnostic Aphasia Examination (BDAE). The “Cookie Theft.”
Broca’s aphasia: Writing • Pts. Write as they speak: slowly and laboriously • Strings of content words sprinkled with misspellings, distortions/omissions of letters. • Poor form, maybe due to hemiplegia (forced to use non-dominant hand) • Usually print; not cursive; slanted writing
Broca’s: comprehension • Comprehension is better than speech or write • Although Broca’s pts tend to be slow readers (careful testing will probably show both reading and listening impairments) • Repair strategy is usually preserved, e.g., they make attempts to correct errors in sph or writing
Broca’s comprehension • Tend to be good tx candidates because they are usually cooperative; • error awareness sometimes leads to emotional lability • Usually remember goals from day to day
Wernicke’s aphasia • Also has other names: sensory aphasia, receptive aphasia and posterior aphasia • Salient feature: impaired comprehension of spoken and printed verbal materials • If severe, pt may be unable to comprehend simple spoken or written material • Mild/moderate: get the basic idea but tend to miss the details
Wernicke’s • Often don’t associate sound (or sight) of words and their meanings • Difficulty with semantic distinctions e.g., know difference between small vs. tiny, good vs. wonderful, etc. • Often display problems with short term retention and recall for verbal material • Tend to do poorly on digit recall, recall lists, etc
Wernicke’s • Performance tends to deteriorate when instructions are longer, more verbal
Wernicke’s: speech • Unlike Broca’s, Wernicke’s patients’ speech is usually smooth, even well formed grammatically • Speech seems less effortful; sometimes even long, syntactically correct utterances with proper prosody • May see some delay when there is difficulty with word recall
Speech sounds good, eh? • Not. • Speech is usually typified with verbal paraphasias (sometimes literal paraphasias, too) • Ferbus lalo! Neologisms • Strings of neologisms: jargon • Essentially, Wernicke’s aphasics produce “empty speech” it lacks meaning • Usually filled with “stuff” or “things” or pronouns • Even circumlocute!
Logorrhea • Some Wernicke’s patients will talk copiously until you MUST interrupt them • Due to circumlocution and poor self monitoring skills
Wernicke’s: writing • Yup, it resembles their speech: writing is better in that the letters are well formed, they write with ease and it is legible • Most will use cursive • Handwriting is mechanically normal but ----it lacks content • Paraphasias in speech usually show up in writing, too • Yeah, logorrhea happens in writing, too.
Wernicke’s candidacy • Patients are usually alert, attentive and likely to stay on the task at hand • Mild forms usually know their errors • Moderate forms rarely notice errors nor attempt to repair errors • Can’t stay on task in testing and tx procedures • Conversational speech is tangential
Auditory comprehension problems complicate all communication trials • Pragmatics/turn taking is usually preserved
Concommitants • Wernicke’s patients are not usually hemiplegic (unless there is involvement of the motor strip-- “global aphasia”) • Lesions deep in the temporal lobe may destroy portions of the visual cortex • Causes contralateral visual field loss