Download
1 / 60
680 likes | 1.12k Views
Tularemia. Francisella tularensis. History. Discovered early 20 th century Tulare county, California “deerfly” fever. History. Discovered early 20 th century Tulare county, California “deerfly” fever Bioweapon potential Incapacitating . History. Discovered early 20 th century

E N D
Tularemia Francisella tularensis
History • Discovered early 20th century • Tulare county, California • “deerfly” fever
History • Discovered early 20th century • Tulare county, California • “deerfly” fever • Bioweapon potential • Incapacitating
History • Discovered early 20th century • Tulare county, California • “deerfly” fever • Bioweapon potential • Incapacitating • Former US and USSR production
History • Discovered early 20th century • Tulare county, California • “deerfly” fever • Bioweapon potential • Incapacitating • Former US and USSR production • Prior use • Unit 731, Manchuria
Epidemiology • Distribution • Moderate climates – U.S., Europe, Russia, Japan
Epidemiology • Distribution • Moderate climates – U.S., Europe, Russia, Japan • 125 annual U.S. cases – mostly Midwest
Epidemiology • Distribution • Moderate climates – U.S., Europe, Russia, Japan • 125 annual U.S. cases – mostly Midwest • Zoonosis • Small mammals (rabbits)
Epidemiology • Transmission • Skin contact - e.g. infected animal
Epidemiology • Transmission • Skin contact - e.g. infected animal • Arthropod bite – ticks
Epidemiology • Transmission • Skin contact - e.g. infected animal • Arthropod bite – ticks • Aerosolization - BT attack; lawn mowers
Epidemiology • Transmission • Skin contact - e.g. infected animal • Arthropod bite – ticks • Aerosolization - BT attack; lawn mowers • Mortality • <2% overall, 30-60% untreated pneumonic
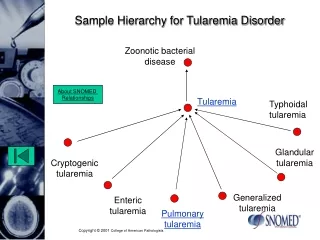
Epidemiology • Forms of disease
Epidemiology • Forms of disease • Pneumonic (<5% of cases) • Expected in aerosol release
Epidemiology • Forms of disease • Pneumonic (<5% of cases) • Expected in aerosol release • Ulceroglandular (45-85%)
Epidemiology • Forms of disease • Pneumonic (<5% of cases) • Expected in aerosol release • Ulceroglandular (45-85%) • Glandular (5-25%)
Epidemiology • Forms of disease • Pneumonic (<5% of cases) • Expected in aerosol release • Ulceroglandular (45-85%) • Glandular (5-25%) • Oculoglandular (<5%)
Epidemiology • Forms of disease • Pneumonic (<5% of cases) • Expected in aerosol release • Ulceroglandular (45-85%) • Glandular (5-25%) • Oculoglandular (<5%) • Oropharyngeal (<5%)
Epidemiology • Forms of disease • Pneumonic (<5% of cases) • Expected in aerosol release • Ulceroglandular (45-85%) • Glandular (5-25%) • Oculoglandular (<5%) • Oropharyngeal (<5%) • Typhoidal (<5-15%)
Microbiology • Pleomorphic Gram negative coccobacillus • Usually not visible in clinical specimens • Small (0.2 m), aerobic • Non-motile, non-sporulating
Microbiology • Pleomorphic Gram negative coccobacillus • Usually not visible in clinical specimens • Small (0.2 m), aerobic • Non-motile, non-sporulating • Fastidious • Slow growth (2-3+ days) • Requires cysteine-enriched media
Microbiology • Pleomorphic Gram negative coccobacillus • Usually not visible in clinical specimens • Small (0.2 m), aerobic • Non-motile, non-sporulating • Fastidious • Slow growth (2-3+ days) • Requires cysteine-enriched media • 2 major strains (A and B) • A predominates in U.S., higher mortality
Pathogenesis • Inoculation of virulent organisms
Pathogenesis • Inoculation of virulent organisms • Local infection at site • Lung – bronchiolitis, pneumonitis, pleuritis
Pathogenesis • Inoculation of virulent organisms • Local infection at site • Lung – bronchiolitis, pneumonitis, pleuritis • Migrate to regional lymph nodes
Pathogenesis • Inoculation of virulent organisms • Local infection at site • Lung – bronchiolitis, pneumonitis, pleuritis • Migrate to regional lymph nodes • Hematogenously seed multiple organs
Pathogenesis • Inoculation of virulent organisms • Local infection at site • Lung – bronchiolitis, pneumonitis, pleuritis • Migrate to regional lymph nodes • Hematogenously seed multiple organs • Suppurative immune response
Clinical Features • All forms of disease • Acute onset • Initial flu-like illness • Fevers, chills, sweats, headache
Clinical Features • All forms of disease • Acute onset • Initial flu-like illness • Fevers, chills, sweats, headache • Lower back myalgias
Clinical Features • All forms of disease • Acute onset • Initial flu-like illness • Fevers, chills, sweats, headache • Lower back myalgias • Incubation 2-5 days (range 1-21)
Clinical Features • All forms of disease • Pulmonary symptoms • Cough, dyspnea, chest pain (40%)
Clinical Features • All forms of disease • Pulmonary symptoms • Cough, dyspnea, chest pain (40%) • Pulse/temperature dissociation (40%)
Clinical Features • Pneumonic form
Clinical Features • Pneumonic form • Symptoms • Nonproductive cough, +/- hemoptysis • Dyspnea, pleuritic pain
Clinical Features • Pneumonic form • Symptoms • Nonproductive cough, +/- hemoptysis • Dyspnea, pleuritic pain • Chest radiograph • Infiltrates – patchy, bilateral • Effusions common
Clinical Features • Ulceroglandular form
Clinical Features • Ulceroglandular form • Ulcer – painful maculopapule, pustule, ulcer
Diagnosis • High index of suspicion
Diagnosis • High index of suspicion • No readily available rapid tests
Diagnosis • High index of suspicion • No readily available rapid tests • Gram stain unhelpful
Diagnosis • High index of suspicion • No readily available rapid tests • Gram stain unhelpful • Gold Standards • Serology (retrospective) • Culture (insensitive, hazardous, slow)
Diagnosis • High index of suspicion • No readily available rapid tests • Gram stain unhelpful • Gold Standards • Serology (retrospective) • Culture (insensitive, hazardous, slow) • Rapid presumptive tests • DFA, IFA, PCR, IHC at reference labs
Treatment • Supportive care • Parenteral antibiotics ASAP • Aminoglycosides • Streptomycin 1 g IM q12°
Treatment • Supportive care • Parenteral antibiotics ASAP • Aminoglycosides • Streptomycin 1 g IM q12° • Gentamicin • Once-daily or traditional dosing
Treatment • Supportive care • Parenteral antibiotics ASAP • Aminoglycosides • Streptomycin 1 g IM q12° • Gentamicin • Once-daily or traditional dosing • Tetracyclines – higher relapse rate • Doxycycline 100 mg IV q12° • Tetracycline - oral
Treatment • Parenteral antibiotics • Others • Chloramphenicol – for meningitis
Treatment • Parenteral antibiotics • Others • Chloramphenicol – for meningitis • Ciprofloxacin
Treatment • Parenteral antibiotics • Others • Chloramphenicol – for meningitis • Ciprofloxacin • Ineffective agents • ß-lactams, macrolides
Treatment • Duration of therapy • 10 (aminoglycosides) – 21 (tetracyclines) days • Switch to oral therapy when clinically improved