Download
1 / 10
100 likes | 232 Views
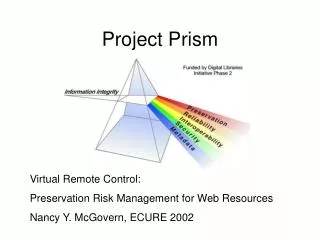
PRISM Predictive Risk Stratification Model Project Leo Lewis National Project Manager Lead for Chronic Conditions Management, Telehealth and Telecare Leo.lewis@ihc.wales.nhs.uk. Definition of Predictive Modelling.

E N D
PRISM Predictive Risk Stratification Model Project Leo Lewis National Project Manager Lead for Chronic Conditions Management, Telehealth and Telecare Leo.lewis@ihc.wales.nhs.uk
Definition of Predictive Modelling “Predictive modelling is a set of tools used to stratify a population according to its risk of nearly any outcome…ideally, patients are risk-stratified to identify opportunities for intervention before the occurrence of adverse outcomes that result in increased health and social care costs.” Cousins MS, Shickle LM, Bander JA. An introduction to predictive modelling for disease management risk stratification. Disease Management 2002;5:157-167 Prism algorithm outcome (dependent variable): “Risk of an individual having an emergency admission to hospital.”
Evidence base and background - PARR tool PARR++ tool – Patients at Risk of Re-hospitalisation: • Algorithm variables derived from secondary care data sets only • Limited to identifying the top 0.1 – 4% of population (‘hospital frequent flyers’) • All NHS Trusts in Wales should run the PARR++ tool regularly • There is no charge for PARR++
Evidence base and background – Combined Predictive Model Combined Predictive Model – England • Developed on limited sample population size – 0.7% • Dependent variable - ‘risk of emergency admission’ • Primary and secondary care data sets: • Full extract of coded data in GP record • 3 year historical extract of Inpatient, Outpatient and A&E data from HES, national Outpatient activity database, and A&E • 69 independent variables from data sets: • Demographics, diagnoses, drugs, NHS utilisation, tests and investigations, unwarranted variations
Prism algorithm • Development work by Health Dialog (PARR and Combined Predictive Model (CPM) developers) • > 10% records sample of population of Wales (vs. 0.7% CPM)) • Stratifying risk across an entire population (vs. 0.1 – 4% of PARR) • Identifying ‘emerging risk’ and clinical opportunities for proactive intervention • Prism algorithm will be validated in four LHBs (vs. 2 in CPM)
General approach Identify diagnoses, procedures, drugs IP, OP, A&E and GP – 69 variables data for prior 24 months Predict any emergency admission next 12 months Dependent Variable Independent Variables Historical Year 1 Year Following Prediction Historical Year 2 Prediction
Where are most of the addressable opportunities in the pyramid?
Stratification across practices supports commissioning decisions and intervention planning
Questions Prism will help to answer • How do I allocate scarce case management resources to achieve maximum benefit? • Combined Model allows for risk stratification across the continuum; identifies ‘emerging risk’ patients; and increases accuracy • Which patients may benefit from a care-co-ordination service? • PRISM will identify all patients in level 3 where co-ordination of care across the sectors could lead to benefits for patients and services • How do I turn precise needs assessment into highly targeted intervention? • Integration of primary and secondary care data sets offers opportunities to build rich clinical profiles to design finely tuned interventions • How can I commission services to achieve maximum savings? • Proportional interventions, reflecting the drivers of risk in different segments, can serve to reduce unnecessary utilisation; improving quality while paying for themselves