Download
1 / 30
360 likes | 667 Views
Total Anomalous Pulmonary Venous Connection. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Total Anomalous Pulmonary Venous Connection. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery.

E N D
Total Anomalous Pulmonary Venous Connection Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
Total Anomalous Pulmonary Venous Connection Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
Total Anomalous Pulmonary Venous Connection • Definition • Cardiac malformation in which there is no direct • connection between any pulmonary vein & left atrium, • but all the pulmonary veins connect to right atrium • or one of it’s tributaries. A PFO or an ASD is present • essentially all persons who survive after birth. • History • Wilson : 1st description in 1798 • Muller : 1st closed partial approach in 1951 • Lewis & Varco : Successful open repair in 1956
Total Anomalous Pulmonary Venous Connection • Origin of anomalous connection • 1. Drainage to right atrium • 2. Drainage to right common cardinal system • (SVC or azygous vein) • 3. Drainage to left common cardinal system • (Left innominate vein or coronary sinus) • 4. Drainage to umbilical-vitelline system • (Portal vein, ductus venosus, and so on)
Pulmonary Vein • Development Splanchnic plexus provides drainage of the lung buds into cardinal & umbilicovitelline venous system. Common pulmonary vein evaginates from the left atrium and merges with the splanchnic plexus. Connections of pulmonary drainage to systemic venous system regress.
TAPVC • Pathophysiology • Entire pulmonary venous return drains into the right atrium, usually via a common pulmonary vein confluence, resulting in complete pulmonary and systemic venous mixing. • Oxygenated blood reaches the left heart via an inter-atrial connection (i.e.,ASD, PFO). • Mechanical or functional obstruction of the pulmonary venous return leads to cyanosis, acidosis, pulmonary hypertension, & congestion.
1. Pulmonary venous anatomy 1) Type : Supracardiac 45% Cardiac 25% Infracardiac 25% Mixed 5% 2) Pulmonary venous obstruction . Junction of connecting vein or compression, or long narrow connect vein . Functional obstruction (restrictive PFO) 2. Chamber & septal anatomy . LA & LV : small . ASD or PFO : small in 1/2, rarely no ASD or PFO 3. Pulmonary vasculature . Increased arterial muscularity . Structural change 4. Associated condition . PDA : 15% . VSD : occasionally . TOF, DORV, IAA : rarely TAPVC • Morphology
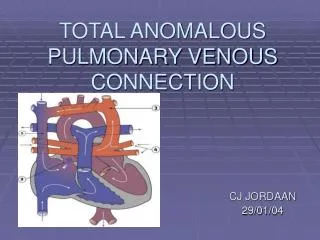
TAPVC • Types
TAPVC • Types
Supracardiac TAPVC Connecting vertical vein Common vein
Cardiac Type TAPVC Common vein
TAPVC • Clinical features & diagnosis • 1. Presentation • . Critically ill infants during 1st few week of life • . Unexplained tachypnea & unimpressive cyanosis • . Metabolic acidosis : pulmonary venous obstruction • 2. Examination • . No particularly overactive heart & unimpressive heart sound • 3. Chest radiography • . Normal heart size with diffuse haziness or ground glass • if pulmonary venous obstruction • . Large heart size with high pulmonary blood flow • . Figure of 8, snowman configuration • 4. Echocardiography • 5. Cardiac catheterization & cineangiography
TAPVC • Natural history • 1. Incidence • . Relatively uncommon anomaly, 1.5~3% of CHD • 2. Survival • . Unfavorable prognosis • 50% survival in 3months • 20% survival in one year • . Usually have pulmonary venous obstruction due to • long pulmonary venous pathway & a small PFO • . Those who survive the first year of life usually have • large ASD, no pulmonary venous obstruction
TAPVC • Indications for operation • Investigation must be undertaken promptly in any neonate or infant, no matter how young, who develops signs or symptoms suggestive of TAPVC • Immediate operation in any neonate or infant whom are importantly ill with TAPVC • Prompt operation in any 6-12 months old infant • Advisable if severe pulmonary vascular disease has not developed in old patients (under 8 units)
TAPVC • Operative techniques • Operation should be undertaken as an emergency after diagnosis by echocardiography who enter the hospital critically ill. Preoperative preparation & stabilization is contraindicated. • 1. TAPVR to Lt. innominate vein • 2. TAPVR to SVC • 3. TAPVR to coronary sinus • 4. TAPVR to right atrium • 5. TAPVR to infradiaphragmatic vein
TAPVC • Supracardiac type
TAPVC • Cardiac type
TAPVC • Infracardiac type
TAPVC Sutureless technique • Suturelesstechnique for the relief of PV stenosis. A, Theincision is made into the left atrium and extended into both upper and lower PVostia separately. B, Suturing is begun in thepericardium just above the junction of the superior PV with the left atrium. C, A second inferior suture is started below theinferior PV and continued in the same manner to the left atrial incision to jointhe superior suture line.
Primary Sutureless Repair • Rationale • Small size of the pulmonary vein is a major risk factor forlater development of PVS after conventional TAPVD repair andthat high mortality of right atrial isomerism is related, at least in part, tointrinsically small pulmonary veins. • Furthermore,most of the patients with RAI are not anatomic candidates forbiventricular repair. PVS is a risk factor for poor Fontan operationoutcome • The acute anatomic benefit for the suturelessrepair is that each vein is its own native size, without anysuture material to cause an excessive inflammatory reactionor luminal compromise
1. Survival 2. Modes of death . Hypertensive crisis . Pulmonary venous stenosis 3. Incremental risk factors for death . Infracardiac drainage . Pulmonary venous obstruction . Poor preoperative state . Small size of pulmonary vein . Increased PVR . Small left ventricle 4. Functional status 5. Hemodynamic result 6. Cardiac rhythm 7. Reoperation . Anastomotic stricture (5~10%) . Pulmonary vein stenosis TAPVC • Surgical results
TAPVC • Special situation & controversies • 1. Delayed operation • In critical patients with obstruction at atrial level, • balloon dilation and 1-2 days later operation • 2. Mixed total anomalous venous connection • 3. Operative exposure • 4. Surgical enlargement of left atrium • Decrease in atrial volume of more than 50% • result in reduction in cardiac output ? • 5. Pulmonary vein stenosis
Residual TAPVC • PVD in remained anomalous veins • Possible pressure-sensitive receptors at the anomalous vein-vena cava junction • Axon reflex triggered by right atrial • distention • Results of the increased blood flow
Pulmonary Vein Stenosis • Etiology • 1. Low grade venous obstruction presents at the • end of procedure results in reactive fibrosis • ( diffuse fibrosis & thickening of vein ) • 2. Self perpetuating stenosis • 3. Intraatrial thickening • 4. Diffuse pulmonary vein stenosis • 5. Congenital nature ( hypoplasia, focal stenosis, • discrete ostial stenosis)
Pulmonary Vein Stenosis • Factors of development • 1. Small confluent pulmonary vein • 2. Suture material • 3. TAPVC type? • 4. Undue trauma toward pulmonary • vein ostium and tension • 5. Steroid therapy
Congenital PV Stenosis • Clinical features • Occur in about 0.4% of congenital heart defects and one or multiple veins may be affected. • Histologically, the lesionis characterized by fibrous intimal thickening in most casesand medial hypertrophy in many • The first surgical repairof congenital PV stenosis was reported by Kawashima and colleaguesin 1971 and surgical approaches have evolved over the years,but results have been generally disappointing. • Diffuse restenosishas been documented as a significant cause of late mortalityafter repair
Acquired PV Stenosis • Characteristics • Anatomically localized to the anastomosis,and the natural history is more favorable, or thestenosis may extend diffusely into the branch pulmonary veins. • It can sometimesbe difficult to distinguish these forms of acquired PV stenosisat the time of presentation. • Acquired PV stenosis occurs inapproximately 7% to 11% of early survivors after total anomalouspulmonary venous connection repair • Results of repairof acquired PV stenosis have also been less than optimal dueto the problem of restenosis
Acquired PV Stenosis • Anatomic features • Post-repair pulmonaryvein stenosis appears to have three basic subtypes. • The mostminimal form of the disease is limited to the anastomotic areawith sparing of the pulmonary veins and confluence, suggestinga technical error or imperfection at the time of initial repair. • The intermediate form is limited to the pulmonary venous confluencein addition to the anastomotic area. • The most extensiveform of the disease includes a fibrous reaction extending retrogradedeep into the lung parenchyma.
Pulmonary Vein Stenosis • Strategy for treatment 1. Minimize trauma at suture line Suture line (tension or inflexibility, deformation) Suture material Handling the vein tissue • 2. Avoid postoperative turbulence • Constraints imposed by restrictive characteristics • 3. Surgical methods • Operative patch venoplasty • Sutureless pericardial marsupialization • Catheter dilation • Stent placement and combination
Complex TAPVC • Etiology of high mortality • 1. The interplay of systemic shunt with abnormal • pulmonary vasculature contributes to difficulty in • maintaining postoperative pulmonary to systemic • flow ratio. • 2. To limit excessive pulmonary blood flow with banding, • or augmentation with shunt, the end result is similar. • 3. The static matching of this resistance to the cardiac • output in face of abnormal pulmonary vasculature may • not allow appropriate regulation of pulmonary blood • flow during dynamic changes.