Download
1 / 76
760 likes | 886 Views
Review Of New CPT Codes Affecting BMT Services. Presented by: James L. Gajewski, M.D.

E N D
Review Of New CPT Codes AffectingBMT Services Presented by: James L. Gajewski, M.D.
Disclaimer: Please note that the opinions expressed in this presentation are those of the presenter and, as such, are intended as guidance only. As always, final interpreta-tion of the requirements of any code, including the acceptability of billing and documentation practices, rests in the domain of the private payer or authorities of the Centers for Medicare and Medicaid Services.
Overview • Background • Review new codes and CMS issues • Critical care E&M issues • Future concerns
Abbreviations • CPT = Current Procedural Terminology • RVU = Relative Value Units • HCPCS = Healthcare Common Procedure Coding System
Committees • CPT Editorial Panel • RVU-RBRVS Update Committee (RUC) • Outpatient Practice Expense – Practice Expense Allocation Committee (PEAC)
Coalition To Address Coding Deficiencies • Sponsor: American Society of Hematology • Co-Sponsors: • American Society for Blood and Marrow Transplantation • American Association of Blood Banks • International Society of Cellular Therapy • The National Marrow Donor Program • American Society of Clinical Oncologists • American Red Cross • Exempt Cancer Centers Committee • Foundation for Cellular Therapies
New Billing Regulations One price per CPT code per patient bill
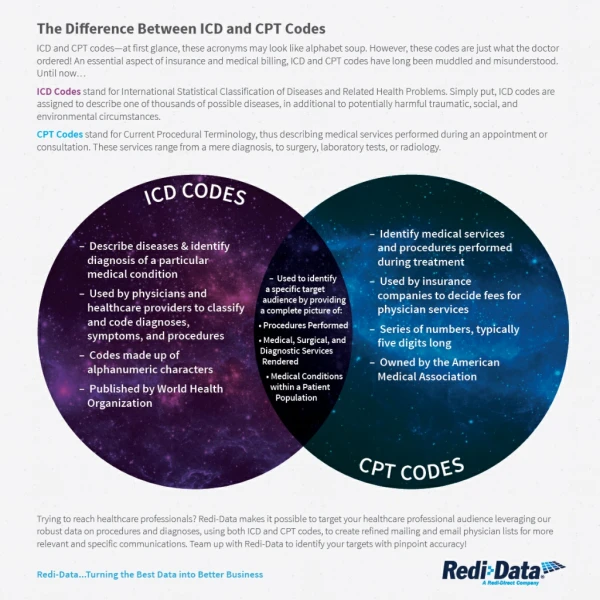
Old Codes Are Inadequate • Apheresis Apheresis Plasma Pheresis • Cell Processing T- and B-cell Removal 86915; Cross-reference to 88240 and 88241 for cryopreservation and thawing
CPT editorial committee has been trying to enhance “granularity” of CPT • Most patient bills need either HCPCS Level I better known as CPT codes OR • HCPCS Level II codes attached to services for electronic billing of services
Review Of New Codes • Rationale behind request • Facility related expenses • Physician professional component • Documentation necessities
Apheresis • Therapeutic apheresis: • 36511 For white blood cells • 36512 For red blood cells • 36513 For platelets • 36514 For plasma pheresis • 36515 With extracorporeal immunoadsorption and plasma reinfusion • 36516 With extracorporeal selective adsorption or selective filtration and plasma reinfusion
ApheresisRationale • Different costs of disposables for different procedures • Different types of personnel using procedures that are commonly performed on emergent basis • Different level of physician involvement for different procedures
ApheresisFacility Related Expenses • All apheresis codes are billed as facility based • Each procedure has separately priced disposables • Each code has the appropriate technical component to assure appropriate billing • e.g. time for performing a white blood cell or plasma exchange may be greater than a red blood cell or platelet exchange
ApheresisFacility Related Expenses • For governmental payers, these procedures can only be billed from hospital based inpatient or outpatient facilities • Project for future is PEAC survey for these services so that free standing facilities can bill governmental payers
ApheresisPhysician Professional Component • Physician work effort surveys were done but RUC did not approve of the surveys • Each apheresis procedure has an RVU of 1.74 • The RVU for 36516 may be decreased to 1.22 in 2004
ApheresisProfessional Billing Criteria • Procedural professional fee does not require physician to do procedure, but requires physician to examine patient during procedure and demonstrate active supervision of procedure. • Physician must be available. Available means within hospital during entire procedure. This does not mean the physician must remain in pheresis unit.
ApheresisProfessional Billing Criteria • Evaluation of patients for apheresis is billable separately as long as it is done on a different day. This is billed on consult H&P. • Post-procedure follow-up is also billable separately as long as it is done on a different day, following E&M service. • For inpatients, different physicians from same specialty may bill service on the same day. Hematologists follow acute leukemia on inpatients and different hematologists perform apheresis procedures.
Billing for apheresis services would be easier if apheresis was recognized as a unique specialty!
Donor Search and Transplant Product Acquisition • 38204 Management of recipient hematopoietic progenitor cell donor search and cell acquisition
Donor Search and Transplant Product Acquisition – 38204Physician Professional Component • For physician supervision of donor search coordinators identifying an unrelated donor and communicating with donor center medical directors and the harvesting physicians. This code is also to be used for cord blood searches. Patient contact is not necessary for this code to be billed.
Donor Search and Transplant Product Acquisition – 38204Facility Related Expenses • This donor search CPT code may not be used for NMDP/Cord Blood Registry donor services on product acquisition. • On patient bills, these services should either have no CPT attached or a generic CPT code such as 38999. • Future task is to create HCPCS Level II codes for these services.
Donor Search and Transplant Product Acquisition – 38204Facility Related Expenses • The donor search code will usually be billed once. This may be billed for successful and unsuccessful searches. • If a search goes to BMT, the BMT fails and a new search is done for a new donor, this code may be billed twice. • If a DLI or boost from the same donor is used, then this code may not be billed twice.
Donor Search and Transplant Product Acquisition – 38204 • Medicare chose not to recognize this code. Medicare felt the service should be valued under infusion CPT 38240. • Appeal is underway.
Stem Cell Collection • 38205 Blood derived hematopoietic progenitor cell harvest for transplantation; allogeneic • 38206 Blood derived hematopoietic progenitor cell harvest for transplantation; autologous
Stem Cell Collection – 38205 & 38206 Rationale • The old codes were split due to expenses for donor evaluation
Stem Cell Collection – 38205 & 38206Facility Related Expenses Both codes cover the collection services for one day’s collection. Multiple day’s services require multiple uses of this code.
Stem Cell Collection – 38205 & 38206Facility Related Expenses • For governmental payers, i.e. Medicare or Medicaid, these services are facility based. • They can only be billed from hospital based inpatient or outpatient collection facilities. This does not apply to non-governmental payers. • If we try to make these codes not-facility based, the issue is whether nurse time can be attached to practice expense or must be allocated to professional fee. This needs to be better understood before doing a PEAC survey
Stem Cell Collection – 38205 & 38206Suggested Facility Related Expenses • The pricing of the service may include: Nurse/technician time, machine disposables, machine depreciation, space utilized and all costs associated with meeting regulatory requirements.
Stem Cell Collection – 38205 & 38206Physician Professional Component • Physicians may bill for this procedure even if not doing the procedure. RVU valuation was for physician supervision of nurse/ technician performing the procedure. To bill, the physician must document exams during procedures and supervision of staff for a particular patient. Physician must remain within hospital for entirety of procedure and be immediately available. The physician does not need to be in the apheresis unit for entirety of procedure. • This is a per-day physician charge for management of collection. For multiple day collections, these codes may be be billed on multiple days.
Allogeneic Stem Cell Collection – 38205Physician Professional Component • Allogeneic donor assessment for apheresis should be new patient – not consult H&P (there is not referring physician). • Follow-up after care on a different day may use follow-up E&M codes.
Autologous Stem Cell Collection – 38206Physician Professional Component • Autologous pre-stem cell collection may be billed as a consult H&P if the physician doing apheresis is different from the physician managing the cancer care. This can be a “within specialty” consult; however, this consult cannot be done on the day of collection. Wording of consult is important-or it will be a referral-transfer of care. • Autologous post-proceeding assessment is billable by E&M codes for follow-up as long as by different physicians doing routine cancer care. This cannot be billed on the day of collection.
Cell Processing Rationale • Allow granularity for cell processing so that we do not utilize the old 86915 for red blood cell depletion • Codes moved to join other BMT related codes in CPT manual • Removed reference to 88240 and 88241 which were designed for laboratory diagnostic procedures not therapeutic transplant services
Cell Processing Codes Rationale • CPT would only give codes to procedural processes that are accepted • T-cell depletion and tumor purging have codes but not CD34 selection • Stem cell expansion still in research and we cannot set code for this service
Cell ProcessingGeneric Facility Pricing Issues • These are per day codes • Markets sets prices, but in assessing cost to determine institutional pricing consider including: • Technician time, supplies, machine use, machine depreciation, space costs, malpractice risk, quality assurance testing of an individual product, overhead • Pricing may include amortization of GMP laboratory construction cost but must be amortized over 10 years • RVU-RBRVS Committee established temporary RVU’s for all of these codes, but CMS chose not to recognize these rvu’s
Cell ProcessingPhysician Work Effort • Includes: • Review of data important for cell processing decisions • Supervision of technicians performing an individual patient’s cell processing • Review and interpretation of quality assurance procedures for an individual patient’s cells being processed, including flow cytometry • Report on product adequacy and ability of cellular product to meet expectations • Time for report preparation and review of cell processing • Malpractice risk • Psychological stress
Cell Processing 38207 Transplant preparation of hematopoietic progenitor cells; cryopreservation and storage
Cell Processing – 38207Suggested Facility Related Expenses • For cryopreservation and storage of bone marrow or peripheral blood progenitor cells. • Facility fees include tech time, laboratory supplies, machinery, machinery depreciation, and space costs. • If mononuclear cell processing was done prior to cryopreservation, it should be billed separately. • Cryopreservation charge should include all quality assurance testing. • After 2004, this code will include billing for all flow cytometry tests used for quality assurance testing.
Cell Processing – 38207Physician Professional Component • Planning for cryopreservation • How many stem cells or T-cells will be stored to meet needs of transplant? • What are anticipated issues? • Donor-recipient HLA/ABO/infectious disease serology, recipient/donor size disparity • What is RBC contamination of product? • Which quality assurance procedures will be performed? • CD34, CD3 tests • Microbiology testing • Technician supervision • Review of freezer curves • Report generation to review adequacy of cryopreserved product and the product’s ability to meet specifications
Cell Processing 38208 Transplant preparation of hematopoietic progenitor cells; thawing of a previously cryopreserved progenitor cell harvest
Cell Processing – 38208Suggested Facility Related Expenses • For thawing of harvest on the day of infusion • Includes all equipment, equipment depreciation, space costs, and technician time used in thawing process • Post thaw viability testing
Cell Processing – 38208Physician Professional Component • Includes: • Review of patient/donor data, freezer curves, adequacy of cryopreserved product • Supervision of thawing, quality assurance testing of pre- and post-thaw product i.e. viability testing flow cytometry (obviously this does not hold up thaw) • Need for special procedures for thawing processes i.e. need for wash; concerns for incompatible RBC contamination • Report on product adequacy and ability to meet specifications • Preparation time for a thaw report • After 2004, flow cytometry will not be billed separately
Cell Processing 38209 Transplant preparation of hematopoietic progenitor cells; washing of a previously cryopreserved progenitor cell harvest
Cell Processing – 38209Rationale and Suggested Facility Fee Issues • For 2003, this is only for thawed cells requiring a wash to remove DMSO • Facility fee should include technician time, machinery, supplies and machinery depreciation • Post-wash viability testing • In 2004, this code will be redesigned for thawing without wash and thawing with wash
Cell Processing – 38209Physician Professional Component • Technician supervision of process • Quality assurance of product after wash • Report generation to review adequacy of product and product’s ability to meet transplant specifications
Cell Processing 38210 T-Cell Depletion
Cell Processing – 38210Suggested Facility Related Expenses • Facility fees may include machinery, machinery depreciation, technician time, supplies, space costs, and quality assurance testing • If cryopreservation is needed, it may be billed separately • If mononuclear cell separation not usually done prior, then may be billed separately • Tests to evaluate efficacy of T-cell depletion • Tests to evaluate viability after T-cell depletion • In 2004, will include flow cytometry testing, pre and post
Cell Processing – 38210Physician Professional Component • Assess donor/recipient suitability for T-cell depletion • Assess HLA typing, donor/recipient size disparity • Assess quality of product coming to lab for T-cell depletion, cell number, CD34 count, CD3 counts • Supervision of technician performing processing • Assessment of efficacy of T-cell depletion • Review and interpretation of quality assurance testing • Report preparation on quality of product to meet specifications
Cell Processing 38211 Tumor cell depletion