Download
1 / 1
70 likes | 412 Views
*Jamie Roper DO & John M Pester DO * St Luke’s University Hospital, Bethlehem PA *Department of Emergency Medicine. Case Presentation. Introduction. HPI 22 yo , 55kg, F 1 day Debilitating 10/10 right sided stabbing/throbbing intermittent HA

E N D
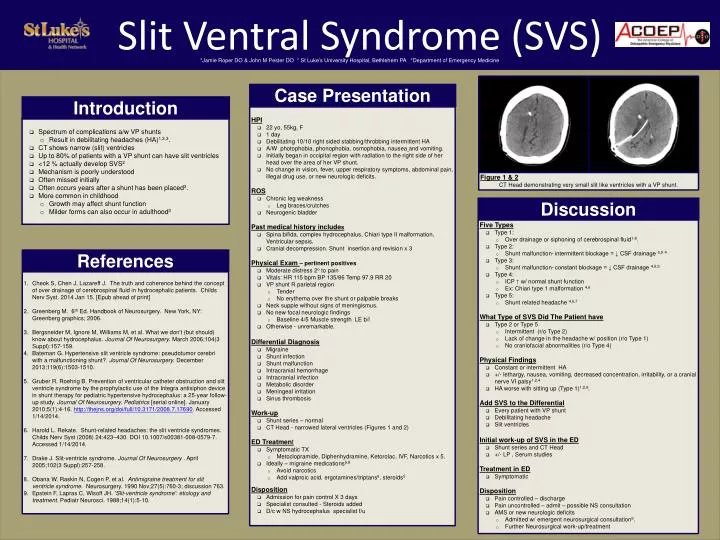
*Jamie Roper DO & John M Pester DO * St Luke’s University Hospital, Bethlehem PA *Department of Emergency Medicine Case Presentation Introduction • HPI • 22 yo, 55kg, F • 1 day • Debilitating 10/10 right sided stabbing/throbbing intermittent HA • A/W photophobia, phonophobia, osmophobia, nauseaand vomiting. • Initially began in occipital region with radiation to the right side of her head over the area of her VP shunt. • No change in vision, fever, upper respiratory symptoms, abdominal pain, illegal drug use, or new neurologic deficits. • ROS • Chronic leg weakness • Leg braces/crutches • Neurogenic bladder • Past medical history includes • Spina bifida, complex hydrocephalus, Chiari type II malformation, Ventricular sepsis. • Cranial decompression. Shunt insertion and revision x 3 • Physical Exam – pertinent positives • Moderate distress 2o to pain • Vitals: HR 115 bpm BP 135/86 Temp 97.9 RR 20 • VP shunt R parietal region • Tender • No erythema over the shunt or palpable breaks • Neck supple without signs of meningismus. • No new focal neurologic findings • Baseline 4/5 Muscle strength LE b/l • Otherwise - unremarkable. • Differential Diagnosis • Migraine • Shunt infection • Shunt malfunction • Intracranial hemorrhage • Intracranial infection • Metabolic disorder • Meningeal irritation • Sinus thrombosis • Work-up • Shunt series – normal • CT Head - narrowed lateral ventricles (Figures 1 and 2) • ED Treatment • Symptomatic TX • Metoclopramide, Diphenhydramine, Ketorolac, IVF, Narcotics x 5. • Ideally – migraine medications6,8 • Avoid narcotics • Add valproic acid, ergotamines/triptans6, steroids5 • Disposition • Admission for pain control X 3 days • Specialist consulted - Steroids added • D/c w NS hydrocephalus specialist f/u • Spectrum of complications a/w VP shunts • Result in debilitating headaches (HA)1,2,3. • CT shows narrow (slit) ventricles • Up to 80% of patients with a VP shunt can have slit ventricles • <12 % actually develop SVS2 • Mechanism is poorly understood • Often missed initially • Often occurs years after a shunt has been placed3. • More common in childhood • Growth may affect shunt function • Milder forms can also occur in adulthood3 Slit Ventral Syndrome (SVS) Figure 1 & 2 CT Head demonstrating very small slit like ventricles with a VP shunt. Discussion • Five Types • Type 1: • Over drainage or siphoning of cerebrospinal fluid1-8. • Type 2: • Shunt malfunction-intermittent blockage = ↓ CSF drainage 6,94 • Type 3: • Shunt malfunction-constant blockage = ↓ CSF drainage 4,6,9 • Type 4: • ICP ↑ w/ normal shunt function • Ex: Chiari type 1 malformation 4,6 • Type 5: • Shunt related headache 4,6,7 • What Type of SVS Did The Patient have • Type 2 or Type 5 • Intermittent (r/o Type 2) • Lack of change in the headache w/ position (r/o Type 1) • No craniofacial abnormalities (r/o Type 4) • Physical Findings • Constant or intermittent HA • +/- lethargy, nausea, vomiting, decreased concentration, irritability, or a cranial nerve VI palsy1,2,4 • HA worse with sitting up (Type 1)1,2,6. • Add SVS to the Differential • Every patient with VP shunt • Debilitating headache • Slit ventricles • Initial work-up of SVS in the ED • Shunt series and CT Head • +/- LP , Serum studies • Treatment in ED • Symptomatic • Disposition • Pain controlled – discharge • Pain uncontrolled – admit – possible NS consultation • AMS or new neurologic deficits • Admitted w/ emergent neurosurgical consultation6. • Further Neurosurgical work-up/treatment References • Cheok S, Chen J, Lazareff J. The truth and coherence behind the concept of over drainage of cerebrospinal fluid in hydrocephalic patients. Childs Nerv Syst. 2014 Jan 15. [Epub ahead of print] • Greenberg M. 6th Ed. Handbook of Neurosurgery. New York, NY: Greenberg graphics; 2006. • Bergsneider M, Ignore M, Williams M, et al. What we don't (but should) know about hydrocephalus. Journal Of Neurosurgery. March 2006;104(3 Suppl):157-159. • Bateman G. Hypertensive slit ventricle syndrome: pseudotumor cerebri with a malfunctioning shunt?. Journal Of Neurosurgery. December 2013;119(6):1503-1510. • Gruber R, Roehrig B. Prevention of ventricular catheter obstruction and slit ventricle syndrome by the prophylactic use of the Integra antisiphon device in shunt therapy for pediatric hypertensive hydrocephalus: a 25-year follow-up study. Journal Of Neurosurgery. Pediatrics [serial online]. January 2010;5(1):4-16. http://thejns.org/doi/full/10.3171/2008.7.17690. Accessed 1/14/2014. • Harold L. Rekate. Shunt-related headaches: the slit ventricle syndromes. Childs Nerv Syst (2008) 24:423–430. DOI 10.1007/s00381-008-0579-7. Accessed 1/14/2014. • Drake J. Slit-ventricle syndrome. Journal Of Neurosurgery . April 2005;102(3 Suppl):257-258. • Obana W, Raskin N, Cogen P, et al. Antimigraine treatment for slit ventricle syndrome. Neurosurgery. 1990 Nov;27(5):760-3; discussion 763. • Epstein F, Lapras C, Wisoff JH. 'Slit-ventricle syndrome': etiology and treatment. Pediatr Neurosci. 1988;14(1):5-10.