Download
1 / 42
450 likes | 1.09k Views
Topical Therapeutics Update . Adam O. Goldstein, MD Associate Professor University of North Carolina Department of Family Medicine Chapel Hill, NC aog@med.unc.edu. Objectives. Advance knowledge of topical preparations Avoid major pitfalls in topical therapeutics

E N D
Topical Therapeutics Update Adam O. Goldstein, MD Associate Professor University of North Carolina Department of Family Medicine Chapel Hill, NC aog@med.unc.edu
Objectives • Advance knowledge of topical preparations • Avoid major pitfalls in topical therapeutics • Learn two therapeutic reasons to preferentially use creams, lotions, ointments or gels • Improve ability to use topical steroids while avoiding side effects
Acne Antifungal * Antibacterial Anti-inflammatory * Moisturizers Sun protection Hair Psoriasis Eczema Aging Debridement Parasites Warts Topical therapies
Art of Topical Therapeutics- Antifungals • How long should you use topical therapy for mild/moderate tinea corporis? • 7-14 Days beyond symptom resolution (Gupta, Drugs, 1998) • What is a preferred topical treatment to prevent recurrence of tinea versicolor? • Selenium Sulfide 2.5% (Selsun Blue) applied and left on overnight intermittently (1x/month) (Savin, JFP, 1996)
Art of Topical Therapeutics- Antifungals • Are topical antifungals all the same? • Whitfield's ointment (benzoic acid) • Undecylenic alkanolamide (Egomycol®, Mycota®, Dr Scholl's® and others) • Ciclopirox olamine (Batrafen® cream, powder, solution) • Polyenes (not for dermatophytes) • Nystatin (Nilstat® cream, ointment; Mycostatin® cream, ointment, paste) (http://www.dermnetnz.org/index.html)
Art of Topical Therapeutics- Antifungals • Imidazoles • Clotrimazole (Canesten®; Clocreme®; Fungizid®) • Econazole (Dermazole®; Ecostatin®; Ecreme®; Pevaryl®) • Ketoconazole (Nizoral®; Sebizole®) • Miconazole (Daktarin®; Fungo®; Micreme®) • Tioconazole (Trosyd®) • Thiocarbamates • Tolciclate (Tolmicen®) , Tolnaftate (Tinaderm) • Allylamine (higher cure rates and more rapid responses than older topical antifungals for dermatophyte infections) • Terbinafine (Lamisil®) (http://www.dermnetnz.org/index.html)
Art of Topical Therapeutics: Anti-inflammatory • What potential side effect do these topical over-the-counter medications share? • Benzocaine 6% • Diphenhydramine 1% • Neomycin • Benzocaine (brand name Lanacane), diphenhydramine (brand name Benadryl), and neomycin (in brand name Neosporin) = • Potential topical sensitizers. (Coskey, JAAD, 1983)
Art of Topical Therapeutics: Anti-inflammatory • Which OTC lotions help control conditions with pruritus as prominent symptom? • camphor, pramoxine or menthol are particularly useful in treating pruritus • Sarna contains camphor and menthol • Gold Bond contains (menthol): • Pramagel and Prax contain pramoxin
Major pitfalls • Prescribing combination products • topical fungal/corticosteroid preparations • Prescribing insufficient amounts • Choosing wrong vehicles • Choosing wrong steroid classes • too weak, too strong, or too long
Prescribing combination topical fungal/corticosteroid preparations • Lotrisone (cream/lotion) • Betamethasone dipropionate/ clotrimazole • Mycolog II, Mytrex (cream, ointment) • Nystatin/ triamcinolone acetonide
Prescribing combination topical fungal/corticosteroid preparations • Nondermatologists (34%) >> than dermatologists (5%) to prescribe combination products for treatment of common fungal skin infections • Potentialsavings = $10-25 million. (Smith, JAAD, 1998)
Preparations • Creams • Lotions • Ointments • Gels • Pastes and Powders • Soaps • Shampoos, foams & mousse • Dressings • Other (e.g. astringents, collodions, tinctures , emollients)
Creams • Useful for most conditions • Acceptable to most patients • Helps ‘dry out’ moist lesions • Tell patients to rub in well • Topical creams generally more potent than lotions • Because of high water content, preservatives added- (may cause allergy)
Lotions • Useful for scalp and other hairy areas • Spreads over wide areas easily • Cosmetically more acceptable in these areas
Ointments • Ointments generally > potency than creams • “Hydrates” dry, itchy skin • Greasy feel and cosmetically not elegant • May be used at bedtime • May occlude hair follicles • Increase potency by putting under occlusion
Gels • Evaporate quickly • Cosmetically elegant • Useful for most skin conditions • Gels may be irritating d/t alcohol in base
Pastes and Powders • Pastes may be useful in intertriginous dermatitis but are difficult to remove • May contain silicones that act as water repellent • Can be aplied sparingly to protect uninvolved skin • Powders help protect intertriginous areas:
Soaps • Soaps and other cleansing bars are useful to cover large areas of skin • Ex. Acne- • Sulfer soap, benzyl peroxide bars, salicylic acid bars
Shampoos and Foams • Shampoos and foams (mousse) offer cosmetically elegant ($$) formulations (increasing) • Examples: • betamethasone valerate mousse, salicylic acid & tar shampoos
Wet dressings • Superficial debridement macerated skin • Burow's Solution (Aluminum Acetate 1/20, 1/40) • 1 packet in 1 pint water • Soak 6 layers of gauze in solution, wring out and apply for 15 minutes • Change dressing q 3-4 hrs
Tube Sizes to prescribe- (bid application for 10 days) • Face and Neck: 30g • Trunk (Front and back): 60g • One Arm: 30g • One Leg: 60g • One Hand: 15g • One Foot: 30g
Tube Sizes to prescribe • Rule of thumb to estimate how much cream or ointment needed to cover area of body • Rule of 9’S: divide body into 11 areas--head, each arm, anterior chest, posterior chest, abdomen, lumbar/buttocks, half of each leg-- • 2 grams/application cream/area
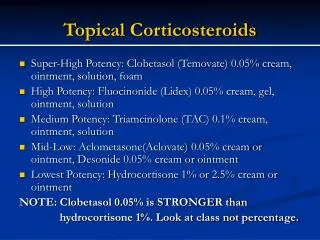
Topical Steroid Potency • Low potency(Hydrocortisone 1%, 2.5%; desonide 0.05%) • Face • Groin • Intertriginous areas • Mid-potency (Hydrocortisone valerate 0.2% cream; triamcinolone acetonide 0.1% lotion, cream; betamethasone dipropionate 0.05% lotion) • Thin skin trunk areas • Extremity lesions
Topical Steroid Potency • High potency (triamcinolone acetonide 0.1% ointment; betamethasone dipropionate 0.05% cream; fluocinonide 0.05% cream) • Thick skin trunk areas • Extremity lesions • Very high/superpotent (fluocinonide 0.05% ointment, betamethasone dipropionate 0.05% ointment; clobetasol propionate 0,05% cream, ointment) • Very thick skinned areas • Palms and soles
Pearls • Potent steroids often effective given 1x/day • Occlusion increases steroid potency x10 • Apply shower cap, plastic bag or saran wrap for stubborn areas • Occlusion increases risks of • atrophy • systemic absorption (Volden, Acta Dermato, 1992)
Potential Adverse Effects of Topical Steroids • Percutaneous absorption and general suppression • Skin atrophy or striae • Papular or perioral dermatitis
Potent Topical Steroids to Face • prolonged (usually >6 weeks) application of potent corticosteroids to the face • rosacea • perioral dermatitis • atrophy
Case 1 • Bob is a 25 year old male who presents with a two month history of worsening itching of his skin. On his initial visit, he presented with the following rash which you diagnosed as eczema. You prescribed him hydrocortisone 2.5% cream, and on follow-up in one week, he states that he is worse. What do you do?
Case 1-answer • Steroid was not strong enough • Consider high potency steroid (triamcinolone acetonide 0.1% ointment; betamethasone dipropionate 0.05% cream; fluocinonide 0.05% cream) for 1-2 weeks, then reduce to medium potency (e.g. triamcinolone acetonide 0.1% cream) • See back in 2 weeks
Case 2 • Margaret is a 52 year old cafeteria worker who was seen by your partner 2 weeks ago with a red, scaly, itchy rash on her hand. She was prescribed samples of a fungal/topical steroid preparation which she took for 10 days. The rash seemed to improve, so she quit taking the medication. It has now returned, and she wonders if she should should continue taking it.
Case 2- answer • DO A KOH SCRAPE TO ENSURE NO FUNGUS • KOH is ---; use a high or ultra potency cream for 2 weeks • Consider if secondarily infected with staph • See back in 2 weeks- if no improvement, consider occlusive therapy
Case 3 • Paul is a 17 year old high school student with acne whom you saw 4 weeks ago for initial acne consult. You prescribed benzamycin and retin A gel. He used the products for 4 days but noticed increasingly intense stinging, redness and irritation of his skin. He stopped the medications and his condition reverted back to his normal skin. What would you do now?
Case 3- answer • Problem: too much, too soon & too irritating • prescription for two products • both gels • too strong strengths • Back off of gels to creams • Use only one formulation for first week
References • Gupta AK, Einarson TR, Summerbell RC, Shear NH. An overview of topical antifungal therapy in dermatomycoses- A North American perspective. Drugs 1998; 55(5):645-74. • Savin R. Diagnosis and treatment of tinea versicolor. J Family Pract 1996; 43(2): 127-32. • Coskey RJ. Contact dermatitis caused by diphenhydramine hydrochloride. J Amer Acad Dermato 1983; 8(2): 204-6. • Smith ES, Fleischer AB, Feldman SR. Nondermatologists are more likely than dermatologists to prescribe antifungal/corticosteroid products: an analysis of office visits for cutaneous fungal infections, 1990-1994. J Amer Acad Dermatol 1998; 39(1): 43-7. • Duweb GA, Abuzariba O, Rahim M, et al. Occlusive versus nonocclusive calcipotriol ointment treatment for palmoplantar psoriasis. Int J Tissue Reactions 2001; 23(2): 59-62.
References • Volden G. Successful treatment of chronic skin diseases with clobetasol propionate and a hydrocolloid occlusive dressing. Acta Dermato-Vener 1992; 72(1): 69-71. • Bruner CR, Feldman SR, Ventrapragada M, Fleischer AB Jr. A systematic review of adverse effects associated with topical treatments for psoriasis. Dermatology Online Journal 2003; 9(1): 2. • Housman TS, Mellen BG, Rapp SR, Fleischer AB Jr, Feldman SR. Patients with psoriasis prefer solution and foam vehicles: a quantitative assessment of vehicle preference. Cutis 2002; 70(6):327-32. • Bikowski J. The use of therapeutic moisturizers in various dermatologic disorders. Cutis 2001; 68(5S):3-11. • Goldstein BG, Goldstein AO. General principles of dermatologic therapy and topical corticosteroid use. UpToDate.com online 2005. • Purdon CH, Haigh JM, Surber C, Smith EW. Foam drug delivery in dermatology. Am J Drug Deliv 2003; 1: 71-75.