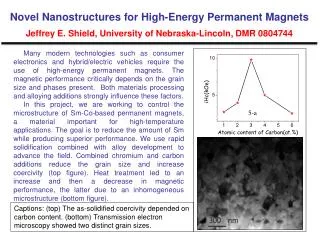
Download
1 / 17
170 likes | 346 Views
Integrating STD Standards of Care into Family Planning Services: Evaluation of chlamydia screening practices and development of a quality improvement intervention. Joan M Chow 1 , Laura J Packel 1 , Linda Creegan 1 , Heidi M Bauer 1 , Jan Treat 2 , Gail Bolan 1

E N D
Integrating STD Standards of Care into Family Planning Services:Evaluation of chlamydia screening practices and development of a quality improvement intervention Joan M Chow1, Laura J Packel1, Linda Creegan1, Heidi M Bauer1, Jan Treat2, Gail Bolan1 1Sexually Transmitted Disease Control Branch, 2Office of Family Planning, California Department of Health Services CDC National STD Prevention Meeting, Philadelphia, March 8, 2004
Presentation Overview • Baseline assessment of chlamydia screening coverage in a large family planning program • Development of provider-specific intervention • Summary of provider feedback about the intervention • Next steps in the evaluation
Background • Chlamydia screening guidelines recommend annual screening of young females • Integration of chlamydia screening standards important in family planning programs • Low screening coverage (<50%) • Programs need to develop • Reliable methods to assess screening • Interventions to improve performance • Evaluate provider screening rate after the provider-targeted intervention
Study Goals & Objectives Study Goal: To improve chlamydia screening rates Study Objectives: • Assess baseline proportion of female clients age 15-25 years screened for chlamydia by specific provider • Inform providers of screening performance plus targeted message
Methods: Assessment of Chlamydia Screening Coverage Program Characteristics: • California Family PACT comprehensive reproductive health program provides family planning and STD services • Eligible: Californians ≤ 200% Federal Poverty Level • Public and private sector providers
Methods: Chlamydia screening estimates Data: • Client enrollment, Medi-Cal provider enrollment, and paid claims data based on fee-for-service • Chlamydia tests identified by CPT-4 codes • Denominator: female clients age 15-25 for FY 2001-2002 • Numerators: Testing in FY 2000/2001 or year before or after
Distribution of chlamydia screening coverage by public vs. private provider type
Methods: Provider Quality Improvement Intervention • June 2003: Clinical Practice Alert and training coupons sent to all Family PACT providers (n~2000) • Sept 2003: Letter with provider-specific CT screening data sent to Family PACT providers who served at least 100 females age 15-25 in FY 01/02 (n=879)
CT Screening Letter Intervention • Low Performance (<50% CT screening) • “Your CT testing rates are well below average and quality improvement activities to improve these rates should be implemented.” • Mid-level Performance (50-79%) • “Your CT testing rates indicate that there is some need for improvement in order to ensure that the majority of young women in your practice are tested.” • High Performance (80% and higher) • “Your CT testing rates indicate that you are doing well in testing the vast majority of young women in your practice. You are to be congratulated. if you would be willing to share methods for implementing a successful CT testing program for young women, we would appreciate hearing from you.”
Provider Telephone Feedback • Providers were encouraged to phone OFP with questions/concerns • Standardized phone contact sheet used to monitor provider concerns • Information collected : • Possible reasons for screening level • Current screening policy • Request for technical assistance
Provider Reported Reasons for Low Screening • Laboratory not billing Family PACT • No pelvic examination performed • Patient refusal • Patient low risk • Patient screened prior to Family PACT enrollment
Screening practices reported by responding providers • Screen only females age 15-25 annually • Screen those with behavioral risk factors regardless of age • Screen everyone routinely including both females ≤ 25 and >25
Limitations to Data • Screening coverage estimates • Paid claims data only • Provider number does not represent an individual provider • Provider intervention • Unknown whether letters actually reached the provider/s • Evaluation of intervention • Preliminary feedback was voluntary
Next Steps: 1) Medical Record Validation of claims data • Sample charts for Family PACT female clients age 15-25 years in FY 01/02 • Identify chlamydia test in past 12 months of current visit • Compare with estimates from claims data 2) Provider evaluation Phone survey of random sample of providers to see if received letter and impact on practice 3) Assess CT screening rates pre- and post-provider-specific CT screening quality improvement intervention
Conclusions • Baseline screening coverage was only 53% • Intervention needed to improve • Provider-specific screening data important for targeting training • <50% screening rate as priority • Dissemination of provider screening data encourages feedback • Annual monitoring of provider screening needed to evaluate impact of letter intervention • Continued quality intervention likely necessary