Download
1 / 53
560 likes | 937 Views
50 YOM blunt trauma by traffic accidence one month ago. 8969424. Unilateral Diaphragmatic Elevation. 1.Subpulmonic pleural effusion dome of pseudodiaphragm migrates toward the costophrenic angle and flattens 2.Altered pulmonary volume (a)Atelectasis

E N D
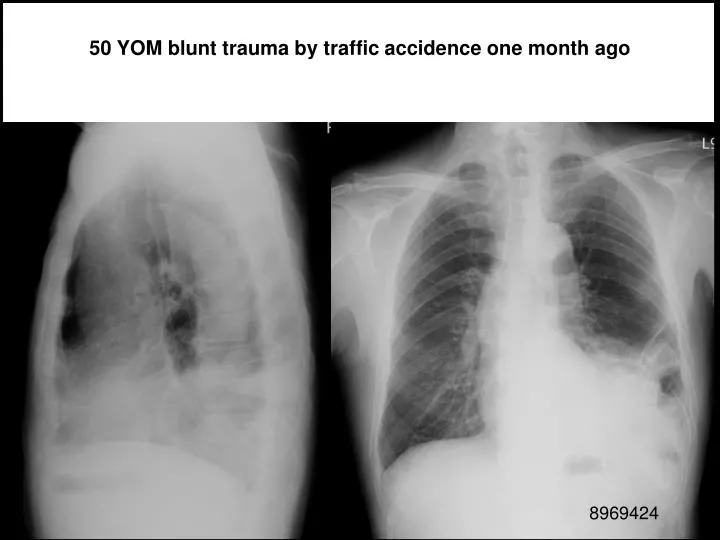
50 YOM blunt trauma by traffic accidence one month ago 8969424
Unilateral Diaphragmatic Elevation 1.Subpulmonic pleural effusion dome of pseudodiaphragm migrates toward the costophrenic angle and flattens 2.Altered pulmonary volume (a)Atelectasis associated pulmonary density (b)Postoperative lobectomy / pneumonectomy rib defects, metallic sutures (c)Hypoplastic lung small hemithorax (more often on the right), crowding of ribs, mediastinal shift, absent / small pulmonary artery, frequently associated with dextrocardia + anomalous pulmonary venous return
3.Phrenic nerve paralysis (a)Primary lung tumor (b)Malignant mediastinal tumor (c)Iatrogenic (d)Idiopathic paradoxic motion on fluoroscopy (patient in lateral position sniffing) 4.Abdominal disease (a)Subphrenic abscess: history of surgery, accompanied by pleural effusion (b)Distended stomach / colon (c)Interposition of colon (d)Liver mass (tumor, echinococcal cyst, abscess) 5.Diaphragmatic hernia 6.Eventration of diaphragm 7.Traumatic rupture of diaphragm Associated with rib fractures, pulmonary contusion, hemothorax 8.Diaphragmatic tumor Mesothelioma, fibroma, lipoma, lymphoma, metastases
Imaging of Diaphragmatic Injury: A Diagnostic Challenge? S. Iochum, T Ludig, F Walter, H Sebbag, G Grosdidier, and AG BlumRadioGraphics 2002; 22: 103S 報告人: 李政家
Anatomy • Central tendon • Crus • Hiatus*3 • Celiac trunk • Inf. Phrenic n.
type 1 configuration(48%). The anterior component is concave posteriorly and continuous with the anterolateral diaphragmatic fibers (arrowheads). • type 2 configuration(28%). The anterior muscle fibers appear to be oriented at an angle in relation to the lateral fibers with midline discontinuity (arrowhead). • type 3 configuration(11%). The anterior muscle fibers lie anteriorly within a single plane.
CT scan shows that the diaphragm is not well demonstrated due to the proximity of the liver, which has the same attenuation. Note the diaphragmatic slips that attach to the ribs (arrowheads). • The coronal and sagittal planes are better than axial planes in analysis of the diaphragm.
Mechanisms of Injuries • Traumatic diaphragmatic injuries occur in 0.8%–8% of patients who sustain blunt trauma. Up to 90% of diaphragmatic ruptures from blunt trauma occur in young men after motor vehicle accidents. • Left hemidiaphragm /right side >3 . right-sided injuries: more underdiagnosis. • Both bilateral tears and extension of tears into the central tendon are uncommon. They are reported in 2%–6% of patients with diaphragmatic injury. • Mechanisms of injuries include a lateral impact, and shears the diaphragm, and a direct frontal impact
Most ruptures are longer than 10 cm and occur at the posterolateral aspect of the hemidiaphragm between the lumbar and intercostal attachments and spread in a radial direction • Penetrating injuries such as gunshot wounds or stab injuries are more random Sites of injuries. Drawing shows radial (A),transverse (B), and central (C) ruptures and a peripheral detachment (D). Radial tears appear to be the most frequently found injury at surgery, whereas peripheral detachments are the least frequent.
Associated Injuries • Common associated injuries include pelvic fractures (40%–55%), splenic injuries (60%), and renal injuries • There is also a high frequency of liver injuries, which are more frequently associated with right than with left diaphragmatic tears. Indeed, liver injuries are seen in 93% of patients with right diaphragmatic injuries and 24% of patients with left-sided lesions • Thoracic injuries such as pneumohemothoraces and rib fractures are seen in 90% of patients. Aortic thoracic injuries are reported in 5% of patients
Various Signs of Diaphragmatic Rupture ---CXR • initial radiographs allow diagnosis of 27%–60% of left-sided injuries but only 17% of right-sided injuries • Specific diagnostic findings: (a) intrathoracic herniation of a hollow viscus (stomach, colon, small bowel) with or without focal constriction of the viscus at the site of the tear (collar sign) (b) visualization of a nasogastric tube above the hemidiaphragm on the left side • Findings suggestive of hemidiaphragmatic rupture include elevation of the hemidiaphragm, distortion or obliteration of the outline of the hemidiaphragm, and contralateral shift of the mediastinum
Left diaphragmatic tear in a 48-year-old man after a motor vehicle accident. Initial chest radiograph shows a gas-filled viscus above the left hemidiaphragm that corresponds to the colon (C). A nasogastric tube is clearly seen in the thoracic cavity (arrow). Left diaphragmatic tear in a 24-year-old woman who was injured in a motor vehicle accident. Initial chest radiograph shows intrathoracic herniation of the stomach (S), a pleural effusion, a pulmonary contusion, and contralateral mediastinal shift.
However, concurrent pulmonary abnormalities related to the trauma such as pleural effusion, pulmonary contusion or laceration, atelectasis, and phrenic nerve palsy can mimic or mask diaphragmatic injury on chest radiographs. In addition, the positive pressure of ventilatory support may delay herniation of abdominal contents through a torn diaphragm • The rate of missed diaphragmatic rupture on chest radiographs ranges from 12% to 66% with the potential risk of a late visceral herniation through the diaphragmatic defect
Various Signs of Diaphragmatic Rupture ---CT • Conventional CT has a variable sensitivity of 14%–61% and specificity of 76%–99% in the diagnosis of diaphragmatic rupture • Helical CT has proved to be more valuable in the detection of diaphragmatic injuries with a sensitivity of 71% (78% for left-sided injuries and 50% for right-sided injuries), a specificity of 100%, and an accuracy of 88% for left-sided injuries and 70% for right-sided injuries. • Moreover, because of the high frequency of associated injuries with blunt diaphragmatic tears, most hemodynamically stable patients with suspected diaphragmatic injuries require an admission CT examination to evaluate the extent and anatomic sites of coexisting thoracoabdominal injuries to guide clinical management.
Findings suggestive of hemidiaphragmatic tears • Direct discontinuity of the hemidiaphragm: sensitivity 73%, specificity 90%. • Intrathoracic herniation of abdominal contents: sensitivity 55%, specificity 100%. • The collar sign: sensitivity 36% with conventional CT 63% with helical CT • On the right side, the collar sign can appear as a focal indentation of the liver, a subtle sign easily overlooked • The dependent viscera sign: sensitivity: 100%: left-sided 83%: right-sided
Left diaphragmatic tear in a 65-year-old patient after blunt trauma. CT scan obtained at the level of the hepatic hilum shows a defect in the continuity of the anterolateral left hemidiaphragm (arrows).
CT scan of the midthoracic region shows intrathoracic herniation of the stomach
Right diaphragmatic tear in a 46-year-old man who experienced multiple injuries in a motor vehicle accident. • CT scan shows a subtle sign of a right diaphragmatic tear: a focal indentation in the posterolateral aspect of the liver with a contusion (arrow).
左: Coronal reformatted image clearly shows a waistlike constriction of the liver (arrowheads).右: Coronal contrast material-enhanced fat-suppressed fast gradient-echo MR image shows a high position of the liver in the thoracic cavity. The constricting rim of the diaphragm is seen as a low-signal-intensity structure around the herniated liver (arrowheads).
Right diaphragmatic tear in a 35-year-old man after a motor vehicle accident. Helical CT scan (direct axial section) shows a focal indentation at the posterolateral aspect of the liver (arrow), a finding suggestive of a right diaphragmatic tear.
左1: Coronal reformatted image shows elevation and focal constriction of the liver. 左2: Sagittal single-shot fast spin-echo MR image clearly shows the posterior diaphragm (arrow), which is outlined by hemoperitoneum and pleural effusion. 右: Coronal contrast-enhanced fast gradient-echo MR image clearly shows waistlike constriction of the liver at the level of the diaphragmatic tear.
Dependent viscera sign in a 28-year-old pregnant woman after a motor vehicle accident. CT scan (direct axial section) shows intrathoracic herniation of the stomach and colon owing to left diaphragmatic rupture, a hepatic hematoma, and a pleural effusion. Note the dependent viscera sign.
Sagittal reformatted image shows a deformity of the aortic contour and an isthmic intimal flap, which indicate an aortic injury.
參考資料 The "Dependent Viscera" Sign in CT Diagnosis of Blunt Traumatic Diaphragmatic Rupture Diane Bergin1, Rachel Ennis, Ciaran Keogh, Helen M. Fenlon and John G. Murray AJR 2001; 177:1137-1140
32-year-old man with left-sided diaphragmatic rupture. Axial CT scan shows discontinuity of left hemidiaphragm (arrows indicate extent of diaphragmatic tear) with gastric and left renal herniation. Stomach lies dependent on left posterior ribs, which is positive "dependent viscera" sign.
32-year-old woman with ruptured right hemidiaphragm. Axial CT scan shows right lobe of liver dependent on right posterior ribs (black arrows), which is "dependent viscera" sign. Partial waistlike constriction (white arrow)—collar sign—is visible along anterior surface of right lobe of liver and is attributable to partial hepatic intrathoracic herniation.
40-year-old man with ruptured right hemidiaphragm. Axial CT scan shows mediastinal shift to left. Right lobe of liver is dependent against right posterior ribs (arrow), a positive "dependent viscera" sign.
58-year-old woman with ruptured right hemidiaphragm. Axial CT scan shows herniation of small-bowel loops, which are dependent against right posterior ribs, a positive "dependent viscera" sign
17-year-old boy with surgically confirmed ruptured left hemidiaphragm. Axial CT scan shows stomach dependent against posterior left ribs (arrow), a positive "dependent viscera" sign.
Pitfalls of CT--- False-Positive • A diaphragmatic defect is not specific for a rupture. Posterolateral defects, which are detected at CT in approximately 6% of asymptomatic adults, may mimic diaphragmatic tears. These defects occur more commonly on the left side and are thought to represent congenital asymptomatic Bochdalek hernias. Acquired diaphragmatic defects are seen more commonly in women, in patients with emphysema, and with increasing age.
Diaphragmatic defects in a 68-year-old patient. CT scans (direct axial sections) show diaphragmatic defects (arrow) of the right (a) and left (b) posterolateral hemidiaphragms
Eventration • a diaphragmatic eventration can mimic a rupture. Coronal and sagittal reformation images are helpful to avoid false-positive diagnosis of diaphragmatic injury and to identify the site of injury
Diaphragm eventration • Incomplete muscularization of the diaphragm. • This very common abnormality consists of a thin membranous sheet replacing the diaphragmatic muscle. • Usually it is partial, involving one half to one third of the hemidiaphragm, frequently the anteromedial portion of the right hemidiaphragm. • The lack of muscle is manifested on the chest radiograph by an elevation of the affected portion of the diaphragm, usually depicted as a smooth hump on the contour of the hemidiaphragm. • When the entire hemidiaphragm is involved, it appears elevated and on fluoroscopy, there is poor, or absent, paradoxical movement. • In many cases, the distinction between this condition and acquired paralysis of the phrenic nerve is impossible
diaphragmatic eventration • upward displacement of abdominal contents secondary to a congenitally thin hypoplastic diaphragm • location: • anteromedial on right • total involvement on the left • R:L = 5:1 • findings: • small diaphragmatic excursions • often lobulated contour
Diaphragmatic paralysis • may be unilateral or bilateral. The most common cause of unilateral paralysis of the diaphragm is involvement of the phrenic nerve by a tumour. But there are many other causes. It occasionally occurs as a complication of various neurological diseases. Also injury to the phrenic nerve as a result of trauma to the thoracic cage or cervical spine and pressure upon the phrenic nerve from a substernal thyroid or aortic aneurysm can cause paralysis. Infectious processes involving the lung, pleura and/or mediastinum may result in temporary or permanent diaphragmatic paralysis. Finally diaphragmatic paralysis can be idiopathic.
The radiological evaluation of diaphragmatic paralysis requires chest radiographs, adequate fluoroscopic tests and clinical information. In some cases chest ultrasonography can also be useful for studying and monitoring diaphragmatic movement. • Four signs indicate diaphragmatic paralysis: • elevation of the diaphragm above the normal range; • diminished, absent or paradoxical movement on inspiration; • mediastinal shift on inspiration; and • paradoxical movement during sniffing (Fig.1).
All these signs need not be present simultaneously but paradoxical movement during sniffing is generally considered as the sine qua non of diaphragmatic paralysis. However, these signs should be interpreted with care since false positive and false negative results occur and other diseases such as lung fibrosis, atelectasis, (hydro)pneumothorax, bronchial stenosis, pneumonia, emphysema and diaphragmatic injury can cause abnormal diaphragmatic position and motion. In addition, the sniff test can be normal in apparently normal patients. Though in these circumstances the paradoxal motion is small (< 2 cm) and predominantly seen in the anterior part of the diaphragm. The radiological diagnosis of bilateral diaphragmatic paralysis can be difficult and the fluoroscopic study of bilateral diaphragmatic paralysis requires simultaneous evaluation of diaphragmatic and chest wall movement.
Isolated elevation of the diaphragm in a 59-year-old man after blunt trauma. (a, b) CT scan (a) and sagittal reformatted image (b) show an isolated elevation of the diaphragm (arrow) without discontinuity. Note the right-sided rib fracture on the scan
Sagittal single-shot fast spin-echo (c) and contrast-enhanced fat-suppressed fast gradient-echo (d) MR images show the diaphragm (arrow) as a thin hypointense band. Fat suppression and contrast enhancement (d) are used for better demonstration of the diaphragm and for differentiation between a pleural effusion and a pulmonary contusion or atelectasis (arrowhead).
Motion artifact in a 28-year-old woman who was involved in a motor vehicle accident. Coronal (a) and sagittal (b) CT reformatted images show an apparent isolated liver herniation due to motion artifact, which could mimic a diaphragmatic tear
Motion artifacts in a 55-year-old woman who was involved in a motor vehicle accident. (a) Coronal CT reformatted image shows motion artifacts. (b) Coronal reformatted image from a shorter CT acquisition with thicker collimation and adequate breath holding shows an intact right hemidiaphragm.
False-Negative • It is frequently difficult to identify the margins of the hemidiaphragm following thoracic trauma because of pleural effusion, particularly in small tears and in the absence of herniation of intraabdominal viscera. • The types of diaphragmatic tears due to blunt trauma are not correlated with the sensitivity of CT for detection of diaphragmatic rupture.
