Download
1 / 21
210 likes | 216 Views
WHO Global Strategy to Reduce the Harmful Use of Alcohol (2010): Background, Outline, Challenges. Thomas F. McGovern, Ed.D . Professor, Psychiatry Stephen Manning, M.D. Assistant Professor, Psychiatry Center for International/Multicultural Affairs March 2, 2011. WHO Strategy (2010). Vision

E N D
WHO Global Strategy to Reduce the Harmful Use of Alcohol (2010):Background, Outline, Challenges Thomas F. McGovern, Ed.D.Professor, Psychiatry Stephen Manning, M.D. Assistant Professor, Psychiatry Center for International/Multicultural Affairs March 2, 2011
WHO Strategy (2010) Vision “To raise global awareness of the magnitude and nature of the health, social and economic problems caused by the harmful use of alcohol, and increased commitment by governments to address the harmful use of alcohol.”
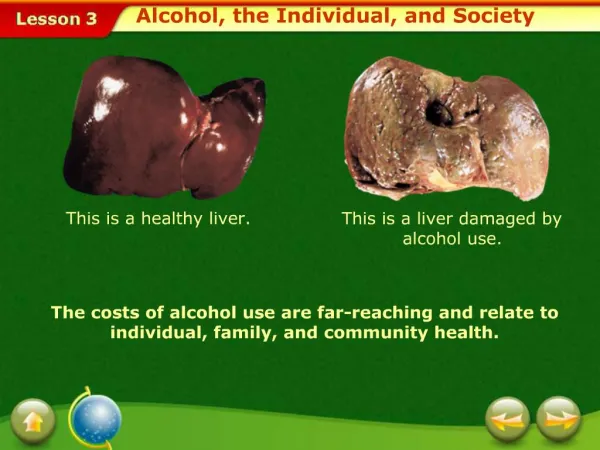
Burden of Disease and Disability 2.3 million died worldwide of alcohol related causes (2002) 3.7% of global mortality in all age groups 4.4% of disability adjusted life years (Dalys) Dalys < Potential years of life lost to premature death > “Healthy life years” lost to poor health/disability (WHO 2004)
Burden of Alcohol Ranks fourth as most modifiable and preventable risk factor for non-communicable disease Health burden for communicable diseases – T.B. and HIV/Aids
The World Medical Association (2008) Alarm Over: Weakening of restrictions on production and marketing of alcohol Changing drink patterns Need for governmental, medical, healthcare interventions (Babor, Zeigler, Chun 2010)
Public Health Research Support the WHO (2010) initiatives Treatment and early intervention Drink-driving countermeasures Limits on availability Restrictions on alcohol marketing, pricing, tax policies to discourage Control on social contexts (Room, Babor or Rehm 2010; Babor and Others 2010)
WHO Global StrategyObjectives Raise global awareness of the magnitude and nature of the health, social and economic problems caused by harmful use of alcohol, and increased commitment by governments to act to address the harmful use of alcohol Strengthen the knowledge base on the magnitude and determinants of alcohol related harm and on effective interventions to reduce and prevent such harm
WHO Global StrategyObjectives Increase technical support to, and enhanced capacity of, Member States for preventing the harmful use of alcohol and managing alcohol use disorders and associated health conditions Strengthen partnerships, provide better coordination among stakeholders and increase mobilization of resources required for appropriate and concerted action to prevent the harmful use of alcohol
WHO Global StrategyObjectives Improve systems for monitoring and surveillance at different levels, and more effective dissemination and application of information for advocacy, policy development and evaluation
WHO Global StrategyTarget Areas Develop leadership with a solid base of awareness and a strong political will and commitment Health services’ clinical and advocacy responses Community mobilization for action to reduce problems and support victims Drink – driving policies and countermeasures for deterrence and the development of measures to create a healthy driving environment
WHO Global StrategyTarget Areas Regulate the public and commercial availability of alcohol Reducing the impact of marketing of alcoholic beverages, especially targeted to youth Pricing policies to reduce underage drinking and to halt progression towards drinking large volumes of alcohol or episodes of heavy drinking, and no influence consumers’ preferences
WHO Global StrategyTarget Areas Harm reduction approaches addressing the negative consequences of drinking and alcohol intoxication Reducing the public health impact of illegal and informal alcohol through quality control, inspection and taxation Monitoring and surveillance
Challenges to Scientific Community Expand evidence base on harmful use of alcohol to include developing countries where consumption is increasing Use scientific research to guide the adoption of effective alcohol policies at national levels (Babor, Zeigler, Chun 2010)
Role of Economic Operations (Alcohol Beverage Industry) Organizations involved in the production, distribution and marketing of alcohol Concerns raised by Global Status Report (2006), expert committees on problems related to alcohol consumption, Second Report (2007) Exercise control over marketing and promotion of alcohol Not impede public health/public policy initiatives
Alcohol Beverage Industry Efforts to influence public policy Maximize its profits – public health policy to reduce harm Promotion/marketing in low income developing countries Absence of effective policy and treatment resources Industry activity in Sub Saharan Africa, South East Asia (Olafsdottir 2008, Bakke Endall 2010)
Clarion Declaration (2008) Initiative of NGO’s and professional societies Identified industry related activities to minimize public health approach to alcohol problems Urges research institutes/individual researchers to reject financial support for alcohol beverage industry (Babor 2009)
International Center for Alcohol Problems (ICAP) Advocates initiatives, industry driven, to lessen many associated with alcohol Efforts to influence public policy to minimize a public health approach to alcohol problems eg. South East Asia, Sub Saharan Africa
International Society of Addiction Journal Editions (ISAJE) Supports the vision, objectives, target areas identified by WHO strategy Identifies conflict of interest concerns in industry sponsored alcohol research Need for common standard for disclosure of conflict of interest in alcohol/addiction research
Limitations of Strategy Lacks of emphasis on coexisting medical and psychiatric comorbidities Biological/pharmacological interventions Psychotherapeutic and recovery group interventions Individual mental health evaluations Family systems approaches
Recovery Team “recovery” does not appear in the strategy Mobilization of indigenous recovery resources, impact local, community and cultural attitudes to alcohol consumption, alcohol related disorders Potential of worldwide recovery advocacy movement, mutual aid societies (William White, Personal Communication 2011)
Conclusion Remarkable, timely, noble document in its intent and vision Enormous global health burden associated with alcohol problems A challenging research agenda, with outreach to developing countries Blue print for evaluating national programs