Download
1 / 24
240 likes | 244 Views
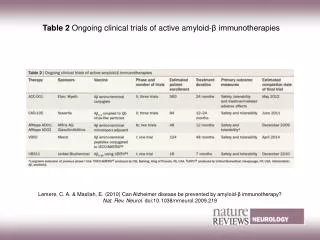
Toxicities and clinical issues with Immunotherapies. Reuben Benjamin King’s College Hospital. Overview of emerging Immunotherapies for Myeloma. Monoclonal antibodies Checkpoint inhibitors Bispecific T-cell engagers ( BiTEs ) CARs, TCR therapy Next generation ImiDs ( CelMods ) Vaccines

E N D
Toxicities and clinical issues with Immunotherapies • Reuben Benjamin • King’s College Hospital
Overview of emerging Immunotherapies for Myeloma • Monoclonal antibodies • Checkpoint inhibitors • Bispecific T-cell engagers (BiTEs) • CARs, TCR therapy • Next generation ImiDs (CelMods) • Vaccines • Allogeneic SCT
Toxicity profile for immunotherapies • Distinct toxicity profile compared with chemotherapy • Mediated by immune activation • Skin: pruritis, rash • Gut : colitis • Liver : autoimmune hepatitis • Endocrine : hypothyroidism • Also immune mediated neuropathy, myositis, arthritis, pneumonitis • Treatment generally with steroids
Toxicity of checkpoint inhibitors in myeloma • Keynote 183 Trial • - Pomalidomide/Dex +/- Pembrolizumabfor relapsed MM ( >2 lines of therapy) • - Number of deaths = 29 (Pembro arm) v 21 (control arm) HR =1.61 at median of 8.1 months • - Grade 3-5 toxicity 83% v 65% • - SAEs 63% v 46% • - ORR 34% v 40%
Toxicity of checkpoint inhibitors in myeloma • Keynote 185 Trial • - Lenalidomide/Dex +/-Pembrolizumabfor upfront treatment of SCT ineligbile MM • - Number of deaths = 19 (Pembro arm) v 9 (control arm) • HR = 2.06 at median of 6.6 months • - Grade 3-5 toxicity 72% v 50% • - SAEs 54% v 39% • - ORR 64% v 62%
Toxicity of checkpoint inhibitors in myeloma • Causes of death in Pembro arm (unrelated to progressive disease) • Myocarditis * • Stevens-Johnson syndrome * • myocardial infarction • pericardial hemorrhage • cardiac failure • respiratory tract infection • neutropenic sepsis • sepsis • multiple organ dysfunction • respiratory failure • intestinal ischemia * • cardio-respiratory arrest • Suicide • pulmonary embolism • cardiac arrest • pneumonia • sudden death • large intestine perforation *
Monoclonal antibodies in myeloma • anti-CD38 • Daratumumab, Isatuximab, MOR202 • anti-CS1 • Elotuzumab • BiTEs • BCMA-CD3 • CD138-CD3
Toxicity of monoclonal antibody therapy in myeloma • Infusion related reactions • 10-71% • Haematological • 20-28% • Interference with laboratory assays • M protein • Indirect antiglobulin test
BiTEs for myeloma • CD3-BCMA antibody • CD3-CD138 antibody • Trials ongoing • ? Expected toxicity similar to Blinatumomab in B-ALL • Infusion reactions • Cytokine release syndrome • Neurotoxicity • Infections
Adoptive T-cell therapy for myeloma • CAR T-cell therapy • TCR therapy • DLI post RIC Allogeneic SCT
CAR-T cell manufacturing process - Autologous CARs - Allogeneic DLI CARs - Off the shelf CARs
Variation in CAR-T cell products • Same antigen target but different scFvs • Different costimulatory domains • CD28, 41BB, 28+41bb • Different gene transfer techniques • Retroviral v lentiviral v non viral • Range of cell manufacturing processes • Autologous v Allogeneic (DLI-CAR) v off-the-shelf CARs
CAR-T cell therapy for myeloma • BCMA CAR • APRIL CAR • CS-1 CAR • CD19 CAR
Complications of CAR-T therapy • Cytokine release syndrome • Neurotoxicity • Infections • Cytopenia • GVHD (with allogeneic CARs)
Cytokine release syndrome • Occurs in 20-40% of CAR treated patients • Fever, malaise, tachycardia, hypotension, capillary leak, renal failure, DIC • Severity related to disease burden • Elevation of serum cytokines • Treatment • aggressive supportive care • IL-6R blockade (Tociluzumab) • Steroids
Neurotoxicity • Occurs in 30-40% of CAR treated patients • Confusion, delirium, aphasia, seizures, coma • Pathogenesis likely cytokine mediated • Treatment • Generally reversible • Supportive care including ventilation • Antiepileptics • Steroids
Cytopenia post CAR therapy • Secondary to lymphodepletion • HLH triggered by cytokine release syndrome • GVHD of marrow (with allogeneic CARs)
Immunotherapy for myeloma - challenges • Identify appropriate patient for a specific immunotherapy • Identify predictive biomarkers for efficacy and toxicity • Refine strategies for early recognition and management of expected and unexpected adverse events • Education and training of clinicians and other health professionals in complications of immunotherapy • Daycare/inpatient capacity
Immunotherapy for myeloma - recommendations • Use Immunotherapy with caution ! • Always think of potential immune related side effects • Perform comprehensive investigations • Serum cytokines • Immune subsets analysis • Biopsy and IHC of affected organ • Appropriate imaging • Involve relevant specialists early • Low threshold for HDU/ICU care • Report/publish all adverse events • Share management strategies through regional/national disease groups