Download
1 / 36
510 likes | 1.14k Views
OnabotulinumtoxinA (Botox®) for the Treatment of Overactive Bladder. Reema Shah Thomas Jefferson University School of Pharmacy Doctor of Pharmacy Candidate March 13, 2013. Objectives. Describe the epidemiology, clinical presentation, pathophysiology , and diagnosis of overactive bladder

E N D
OnabotulinumtoxinA (Botox®) for the Treatment of Overactive Bladder Reema Shah Thomas Jefferson University School of Pharmacy Doctor of Pharmacy Candidate March 13, 2013
Objectives • Describe the epidemiology, clinical presentation, pathophysiology, and diagnosis of overactive bladder • Review the current guidelines for the treatment of overactive bladder in adults according to the American Urological Association • Explain the pharmacology of Botox® • Evaluate the objectives, study design, results, and clinical significance of clinical trials conducted to examine the use of Botox® for the treatment of overactive bladder • Assess the overall risks and benefits of the use of Botox® for the treatment of overactive bladder
Epidemiology • Overactive bladder (OAB) affects 12%-17% of the general population in the U.S. • 1/3rd suffer from urinary incontinence • Higher prevalence rates in women than men • Symptom prevalence and severity tends to increase with age • Significant burden for patients Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022. Tyagi S, et al. UrolClin N Am. 2006. 33: 433-438.
Clinical Presentation • Urinary frequency • >8 micturitions/day • Urgency with OR without urge incontinence • Nocturia • >1 micturition/night or nocturnal incontinence (enuresis) Rovner, et al. Pharmacotherapy: A Pathophysiological Approach. 2008. 1399-1412.
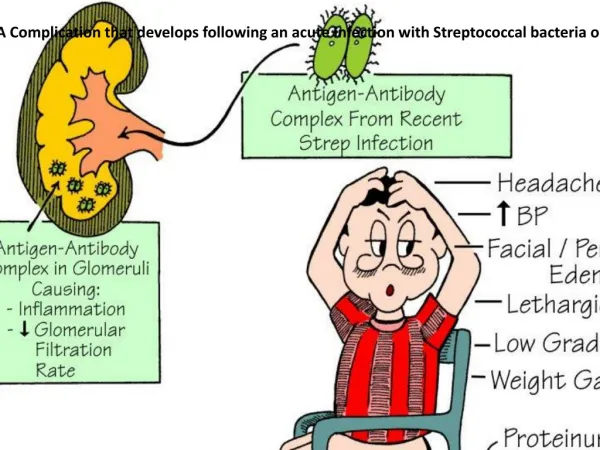
Pathophysiology • Involuntary bladder contractions • Detrusor muscle is overactive and contracts inappropriately during the filling phase • Contraction controlled through activation of muscarinic receptors (primarily M3) by ACh Rovner, et al. Pharmacotherapy: A Pathophysiological Approach. 2008. 1399-1412.
Etiology • Idiopathic (most common) • Normal aging • Neurologic disease • Stroke • Parkinson’s disease • Multiple sclerosis • Spinal cord injury • Myogenic • Bladder outlet obstruction • BPH • Prostate cancer Rovner, et al. Pharmacotherapy: A Pathophysiological Approach. 2008. 1399-1412.
Diagnosis • Based on patient’s symptoms • Urinalysis and urine culture should be negative • rule out urinary tract infection as cause of frequency Rovner, et al. Pharmacotherapy: A Pathophysiological Approach. 2008. 1399-1412.
Current Guidelines for Treatment of Overactive Bladder • 1st /2nd line for treatment: • Nonpharmacological • lifestyle modifications such as toilet scheduling regimens and pelvic floor muscle rehabilitation • Anticholinergic medications • Oxybutynin, tolterodine, trospium, solifenacin, darifenacin • 3rd line for treatment: • Botox® injection Gormley EA, et al. American Urological Association. 2012.
Pharmacology of Botox® • Mechanism of Action • Cleaves SNARE protein • SNAP-25 • Prevents assembly of vesicles • Inhibition of ACh release • Detrusor muscle relaxation • Pharmacokinetics • Onset of action: ~ 2 weeks • Duration: ~ 24 weeks OnabotulinumtoxinA. Lexi-Comp, Inc. 2013. Rowland LP. N Engl J Med. 2002; 347:382-383.
Dosing and Administration • Botox® 100 units reconstituted with 10 ml normal saline • Administered as 20 evenly distributed intradetrusor injections • 0.5 ml per injection site • using a cytoscope • Injections spaced ~ 1 cm apart • Needle inserted ~ 2mm into detrusor • Local anesthesia usually administered into the bladder prior to treatment Botox® [package insert]. Allergan. Irvine, CA; January 2013.
Clinical Trial #1 OnabotulinumtoxinA for the Treatment of Patients with Overactive Bladder and Urinary Incontinence: Results of a Phase 3 Randomized Placebo-Controlled Trial Nitti VW, Dmochowski R, Herschorn S, et al. J Urol. 2012. Purpose: To assess the safety and effectiveness of onabotulinumtoxinA in treating patients with idiopathic overactive bladder with incontinence who were inadequately managed with anticholinergics Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022.
Study Design • Double blind, placebo controlled, randomized trial at 72 sites in the US and Canada • Intention to treat • Patients received one of the following interventions: • Botox® 100 unit intradetrusor injection • Placebo: 10ml normal saline intradetrusor injection • Stratified by site and ≤9 or >9 UUI episodes at baseline • Follow up visits • Occurred at weeks 2, 6, and 12 and thereafter every 6 weeks until exit at week 24 unless retreatment occurred • Retreatment only considered after week 12 Sample population and demographics: • Total: 557 • Botox® = 280 • Placebo: = 277 • Baseline characteristics were balanced across treatment groups • About 90% were female • Average age: 61.3 years • Duration of OAB: about 6.7 years • Prior anticholinergic use: • Duration: 2.4 years • # of anticholinergics: 2.5 • Daily UI episodes: 5.3 • Of those, 4.6 episodes/day were UUI Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022.
Study Design Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022.
Endpoints & Results Primary outcome: • Change from baseline in average UI episodes/day (Weeks 2, 6, 12) • Botox® significantly reduced the daily frequency of UI episodes vs. placebo (-2.65 vs -0.87) • Mean % reductions from baseline of 47.9% with Botox vs. 12.5% with placebo • Analyzed using ANCOVA model • Covariates: baseline value and site • Factor: treatment group Power set at 82% (N=227) to detect a between group difference Significance level=0.05 p <0.001 vs placebo. Error bars are ± 95% CI. Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022.
Endpoints & Results Secondary outcome: • efficacy • All parameters showed statistically significant improvement of outcomes with Botox® use compared to placebo • ↓ micturitionepisodes/day • ↓urgency episodes/day • ↓nocturia episodes/day • ↑volume voided/micturition • Evaluated using ANCOVA P<0.05 Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022.
Endpoints & Results Secondary outcome: • efficacy • HRQOL (week 12) • Incontinence-Specific Quality of Life Instrument (I-QOL) • King’s Health Questionnaire (KHQ) • Use of Botox® significantly improved patients’ HRQOL across all measures compared to placebo • Analyzed using ANCOVA p <0.001 Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022.
Endpoints & Results Secondary Outcome: • Side effect profile (safety) • Most common ADR: UTI (15.5% in Botox® group vs. 5.9% in placebo group) • Urinary retention (5.4% in Botox® group vs. 0.4% in placebo) • Significant increase in PVR urine volume in Botox® group Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022.
Endpoints & Results Secondary outcome: • Proportion of patients who initiated clean intermittent catheterization (CIC) at any time during treatment cycle • 6.1% (17/278) in the Botox® vs. 0% in the placebo group • Protocol: Initiated if PVR urine volume was ≥200ml and <350ml with associated symptoms (voiding difficulties or sensation of bladder fullness) or if PVR urine volume was ≥350ml regardless of symptoms Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022.
Author’s Conclusions • The results of this study suggest that Botox® is an important new alternative treatment option for OAB patients with UI who are inadequately managed by anticholinergic therapy • demonstrated significant and clinically relevant improvements in all OAB symptoms and HRQOL in patients • Overall well tolerated • But high incidence of UTI and urinary retention Nitti VW, et al. J Urol. 2012. doi:10.1016/j.juro.2012.12.022.
Critique of Study Strengths Weaknesses Sponsored/funded by Allergan Failed to mention other medications patient’s were currently on Mostly women took part in trial (~ 90%) • Intent to treat • Randomized • Use of appropriate HRQOL measures • Large sample size
Clinical Trial #2 Anticholinergic Therapy vs. OnabotulinumtoxinA for Urgency Urinary Incontinence Visco AG, Brubaker L, Richter HE, et al. N Engl J Med. 2012. Purpose: • To directly compare/contrast the use of a Botox® injection with the use of an oral anticholinergic for the treatment of urgency urinary incontinence by assessing the reduction in episodes of incontinence, improvement in quality of life, and side effect profiles Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Study Design • 10 center, randomized, double blind, double placebo, controlled trial • Intention to treat Sample population and demographics: • Enrollment: 249 underwent randomization • Anticholinergic group: 126 treated • Botox® group: 121 treated • None of the characteristics differed significantly between the treatment groups • Average age: 56.7-59.3 years • 100% women • 78.5% caucasian • Mean urgency incontinence episodes/day: 5.0 • 41% had not previously received anticholinergic therapy Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Study Design • Assigned into one of the following groups for a period of 6 months: • Oral anticholinergic daily + one time intradetrusor saline injection (placebo) • Solifenacin 5mg PO daily, with possible dose escalation • Oral placebo daily + one time Botox® 100 unit intradetrusor injection • Randomization was stratified according to: • previous exposure or no previous exposure to anticholinergic drugs • baseline severity of UUI • 5-8 episodes vs. ≥ 9 episodes of urgency urinary incontinence in a 3 day period • site Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Study Design Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Study Design Follow Up Evaluation: • Office visits scheduled every 2 months • Patient Global Symptom Control (PGSC) • used to assess whether current treatment was providing adequate control of urinary leakage • Patient’s answered this statement: • “This treatment has given me adequate control of my urinary leakage” • Range from 1 (disagree strongly) to 5 (agree strongly) • Dose escalation was allowed at months 2 and 4 only if • inadequate symptom control (if PGSC score was 1 to 3) • side effects were intolerable • Month 2: switch to solifenacin 10mg daily • Month 4: switch to trospium XR 60mg daily • PGSC score > 3: continue same regimen until next 2 month visit Month 6: • all oral medications were discontinued • Participants that had adequate symptom control and who did not receive off protocol treatment for OAB were followed monthly for up to 6 additional months in order to assess the duration of effect of the medications Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Endpoints & Results Primary outcome: • Mean reduction from baseline in # of episodes of UUI per day over the 6-month, as reported for 3 day periods in monthly bladder diaries • Anticholinergic group: reduction of 3.4 episodes/day • Botox® group: reduction of 3.3 episodes/day • Reduction in episodes per day was similar in the two groups • Evaluated using linear mixed model • P value =0.81 (statistically insignificant) Power set at ≥80% (N=121) to detect a between group difference in reduction of UUI Two sided type 1 error rate of 0.05 (Significance level=0.05) Bars indicate 95% CI Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Endpoints & Results Secondary outcome: (efficacy) • Change in QOL outcomes from baseline • Overactive Bladder Questionnaire (OABq-SF) • Pelvic Floor Distress Inventory (PFDI-SF) • Pelvic Floor Impact Questionnaire (PFIQ-SF) • Patient Global Impression of Improvement (PGI-I) • No statistically significant differences in the magnitude of improvement between both groups P<0.05 Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Endpoints & Results • Secondary Outcome:(safety) • Side effect profile • Statistically significant side effects • -Dry mouth: Higher rates in anticholinergic group (46%) • -# of patients requiring catheterization: higher rates in Botox ® group • -Due to PVR urine volume > 300ml or >150ml in patients who felt moderately bothered • Evaluated using Mantel-Haenszel test Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Endpoints & Results Secondary Outcome: (safety) • Side effect profile • Statistically significant side effects in Botox® group • Urinary tract infection (33%) • Residual volume after voiding >150ml (Urinary retention) P<0.05 Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Endpoints & Results Secondary Outcome: • Duration of effect of medications after cessation of treatment • % of participants with adequate symptom control (PGSC score of 4 or 5) with time • evaluated with the use of Kaplan-Meier product limit estimates and associated log rank tests % of Adequate control of symptoms during off-treatment follow up • 1 month after discontinuation, significantly fewer women in the anticholinergic group than in the Botox® group had adequate control of symptoms • at month 12, results considered insignificant • Duration of effect of Botox is longer Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Author’s Conclusion • No significant difference between oral anticholinergic drug and Botox® injection therapy in regards to: • reduction of the frequency of episodes of urgency incontinence • improvements in quality of life • both were effective treatments and the magnitude of the reductions did not differ significantly between the groups • Choice between these therapies should take into account: • Route of administration • Side effect profile • Anticholinergic: more frequent occurrence of dry mouth • Botox®: higher risks of catheterization because of urinary retention and higher risk of urinary tract infection Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Critique of Study Strengths Weaknesses Did not include patient adherence rates of the oral medications Did not compare cost-effectiveness of the therapies Only women used • No industry support (funding or provision of medications) was received • Randomized, double blind, comparative effectiveness study • Inclusion of possible dose escalation/switching medication • represents usual clinical practice Visco AG, et al. N Engl J Med. 2012. 367:1803-1813.
Clinical Significance • Botox® serves as an effective alternative treatment for overactive bladder withurgeincontinence episodes for patients who have treatment failure with anticholinergic medications • Should not be first line in treatment of OAB due to higher incidence of serious side effects • UTI and urinary retention
References • Nitti VW, Dmochowski R, Herschorn S, et al. OnabotulinumtoxinA for the treatment of patients with overactive bladder and urinary incontinence: results of a phase 3 randomized placebo-controlled trial, J. Urol. 2012. doi:10.1016/j.juro.2012.12.022. • TyagiS, Thomas CA, Hayashi Y, Chancellor MB. The overactive bladder: epidemiology and morbidity. UrolClin N Am. 2006. 33: 433-438. • Rovner ES, Wyman J, Lackner L, Guay,D. Urinary Incontinence. In: Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiological Approach. 7th ed. New York, NY: McGraw-Hill; 2008. 1399-1412. • Gormley EA, Lightner DJ, Burgio, KL, et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. American Urological Association. May 2012. Available at : http://www.auanet.org/content/media/OAB_guideline.pdf. Accessed March 7, 2013. • OnabotulinumtoxinA. In: Lexi-Drugs Online [database on the internet]. Hudson, OH: Lexi-Comp, Inc.; 2013. Available at: http://online.lexi.com. Accessed March 7, 2013. • Rowland LP. Stroke, spasticity, and botulinum toxin. N Engl J Med. 2002. 347:382-383. • Botox® [package insert]. Allergan. Irvine, CA; January 2013. Available at: http://www.allergan.com/assets/pdf/botox_pi.pdf. Accessed March 7, 2013. • Visco AG, Brubaker L, Richter HE, et al. Anticholinergic therapy vs. onabotulinumtoxinA for urgency urinary incontinence. N Engl J Med. 2012. 367(19):1803-13.