Download
1 / 56
560 likes | 991 Views
Peptic Ulcer Disease. 3 月前无明显诱因下出现上腹部疼痛 , 自诉针扎样痛,不剧,多饥饿时好发,进食后可缓解,无他处放射痛,持续 10 多分钟可自行缓解,伴返酸 。 1 月前患者上腹痛加重,为持续性,有夜间发作。未予重视未就诊。 半月前患者无明显诱因下出现黑便, 2 天 1 次。 4 天前患者晚餐后出现呕吐,为胃内容物中带暗红色血块,未见鲜红色血,有头晕乏力,胸闷气促,冒冷汗 , 解黑色大便 2 次。

E N D
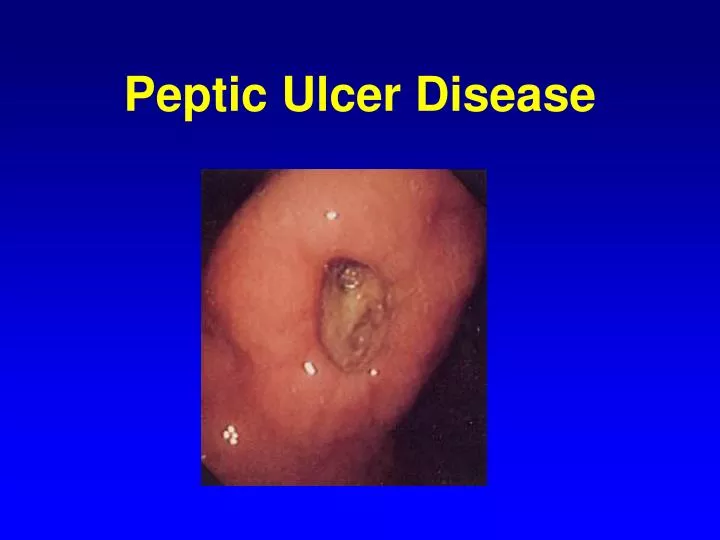
3月前无明显诱因下出现上腹部疼痛,自诉针扎样痛,不剧,多饥饿时好发,进食后可缓解,无他处放射痛,持续10多分钟可自行缓解,伴返酸 。 • 1月前患者上腹痛加重,为持续性,有夜间发作。未予重视未就诊。 • 半月前患者无明显诱因下出现黑便,2天1次。 • 4天前患者晚餐后出现呕吐,为胃内容物中带暗红色血块,未见鲜红色血,有头晕乏力,胸闷气促,冒冷汗,解黑色大便2次。 • 1天前患者再次出现呕血,色鲜红,同时解黑便,伴头晕头痛,呼吸困难,四肢厥冷,遂转我院急诊,急查血常规示血红蛋白3.9g/dl,予静脉补液并输红细胞8u,急诊内镜:“十二指肠球部前壁0.8 X0.8cm溃疡伴出血(A1期)”。
手术记录2010-3-26 • 远端胃大部切除(毕2式吻合)+ 十二指肠残端造瘘 • 探查:十二指肠球部至胃幽门部有质硬的瘢痕组织。十二指肠球部与周围组织粘连严重。于幽门环下约4cm处切断十二指肠,十二指肠残端内放置蘑菇头引流管,并丝线闭合十二指肠残端,用闭合器断胃,距Treiz韧带12cm处提起空肠,于横结肠前行胃空肠端侧吻合,胃小弯对输入袢,置腹腔引流管2根于十二指肠残端附近。
十二指肠溃疡术后8天,呕血8小时 • 患者8天前因十二指肠溃疡术后在我院行急诊远端胃大部切除(毕II式吻合)+十二指肠残端造瘘术。术后无呕血不适,无腹痛腹胀,仍有黑便、低热,其余生命体征平稳,术后7天带腹腔引流管及十二指肠造瘘管转至省青春医院继续治疗。8小时前患者无明显诱因下出现大量呕血,腹腔造瘘管及引流管有血性液体流出,伴腹痛,便血。 • 2010-3-26急诊胃镜:十二直肠球部前壁0.8 X 0.8cm溃疡伴出血,A1期
手术记录 04-03 • 探查:见腹腔内淡红色积液约500ml,腹腔内未见明显新鲜出血,原胃空肠吻合口通畅,未见梗阻,愈合佳,打开残胃前壁,见胃腔内新鲜血液及凝血块约800ml,吸尽血液,检查残胃,未见明显溃疡和出血点,仔细探查见输入袢肠管有新鲜血液流出,输入袢植入胃镜,检查见十二指肠残端内后壁有明显出血点,遂打开十二指肠残端,见残端充血水肿明显,有一活动性出血点,予prolene线缝合止血,后再用胃镜探查整个肠袢无明显出血。冲洗腹腔,彻底止血。置冲洗引流管4根于十二指肠残端附件,一根盆腔引流管,另在胃肠吻合下40cm处置一空肠营养造瘘管,残胃前壁置入蘑菇造瘘管置于输入襻内
手术记录 04-16 • 探查腹腔:腹腔内脏器粘连水肿严重,小肠及结肠内可见大量血凝块,先行粘连松解后,见空肠部分浆肌层缺损,分离暴露十二指肠残端,切开十二指肠残端,见大量鲜血及血凝块喷涌而出,吸除血液及血凝块,见十二指肠残端有一直径大小约为0.8cm溃疡,溃疡内可见一动脉断端鲜血喷出。予proline线沿溃疡缝合后未见明显活动性出血,请术中胃镜,探查十二指肠残端、胃及胃肠吻合口未见明显活动性出血,遂予缝合十二指肠切口,并置入24#蘑菇管1根行十二指肠残端造瘘,切除浆肌层缺损肠段约8cm,行肠肠端侧吻合,十二指肠残端处放置引流管3根。
手术记录 05-01 • 探查腹腔:腹腔内脏器粘连水肿严重,腹腔内结构显示不清,十二指肠水肿明显,先行粘连松解后,沿造瘘管分离暴露十二指肠残端,切开十二指肠残端,见鲜血及血凝块喷涌而出,吸除血液及血凝块,见十二指肠残端后壁内侧有一动脉出血,术中病人心跳骤停,经心肺复苏,心跳恢复,压迫止血,迅速补液输血,予proline线缝合十二指肠出血部位后未见明显活动性出血,肠壁水肿炎症严重无法缝合,予开放,拔除十二指肠残端造瘘管,十二指肠残端处放置引流管4根 。
Pathogenesis “ self-digestion” — Peptic ulcer no acid, no ulcer (no HP, no ulcer?)
Types of Ulcer • I Incisura • II Gastric + Duodenal • III Prepyloric • IV High lesser curve
胃十二指肠溃疡的外科适应证 • ①内科治疗无效的十二指肠溃疡(Refractory ulcer); • ②各种情况的胃溃疡和胃溃疡恶变; • ③急性穿孔; • ④溃疡大出血; • ⑤痕性幽门梗阻; • ⑥应激性溃疡; • ⑦胰源性溃疡。 • Giant Gastric Ulcers >3cm
DuodenalUlcer (DU) Clinical features:节律性、周期性饥饿痛(夜间痛) ca. 30 in age,man>women Acid dyspepsia: the classic ulcer symptom; Burning epigastric pain: Hunger pain (episodic) (2 to 3 hrs after meal),Night pain, Food and alkali relief, Periodicity of the pain: Autumn- early spring; Belching,Heartburn。
十二指肠溃疡 1 、外科手术适应证 (1)严重并发症:急性穿孔、大出血和瘢痕性 幽门梗阻; (2)内科治疗无效(Intractability):顽固性溃疡 病理:慢性穿透性溃疡,球后溃疡。 临床:节律性消失,症状严重,不易止痛, GI:龛影较大(Giant Gastric Ulcers >3cm )、 球部严重变形、穿透出肠 壁外或位于球后 部溃疡者。
十二指肠溃疡 2 、外科手术方法 胃大部切除术 迷走神经切断术
GastricUlcer (GU) • ①小弯溃疡,>50%; • ②高位溃疡; • ③后壁溃疡,多慢性穿透 深入胰腺; • ④复合溃疡 • ⑤幽门前溃疡
GastricUlcer (GU) • Irritable stomach: Indigestion, Dysgastria, • Rule out malignancy, dyspepsia. • >40 years, female:male = 2:1 (sabiston) • 胃痛节律性较不明显。 40~50岁,男性较多 • 进餐后不能很好止痛,餐后1小时疼痛即可开始,持续1~2小时。对抗酸药物疗效不明显。较十二指溃疡容易复发,容易引起大出血、急性穿孔等严重并发症。约有5%胃溃疡可以发生恶变。
Dyspepsia • Pain or Discomfort centred in the upper abdomen
Major structural causes of dyspepsia • Chronic peptic ulcer (duodenal or gastric) • Gastro-oesophageal reflux disease (>50% have no oesophagitis) • Gastric or oesophageal adenocarcinoma (rare but of concern for patient and doctor)
胃溃疡治疗 • 经过8~12周内科治疗无效或愈合后复发; • 年龄 >45岁; • 经X线或胃镜证实为较大(>2.5cm)或高位溃疡; • 不能排除或已证实有恶变者; • 合并或曾有急性穿孔、大出血或梗阻。
Surgical Procedures 一、Subtotal gastrectommy 1 .Billroth-I 2 .Billroth-II 3 .Roux-en-Y 4. Others
Surgical Procedures 1 .Billroth I (1885)
Surgical Procedures 一、Subtotal gastrectomy 1 . Billroth-II
Surgical Procedures 一、胃大部切除术 1 . Roux-en-Y
Surgical Procedures 一、Subtotal gastrectomy 1 .Billroth-I 2 . Billroth-II 3 .Roux-en-Y 4. Others
Surgical Procedures 二、 Vagotomy 1.Truncal vagotomy 2.Selective vagotomy 3.Parietal cell vagotomy (High selective vagotomy)
二、Vagotomy1. Truncal vagotomy迷走神经干切断术2.选择性胃迷走神经 切断木 3.高选择性胃迷走神经 切断术切断:食管裂孔水平左、右二支腹迷走神经干
二、 Vagotomy 2.Selective vagotomy
二、 Vagotomy 3. HighSelective vagotomy Parietal cell vagotomy
Perforation • Free perforation Severe peritonitis,tenderness, rigidity, reboundBoardlike abdomen,Shock. • Contained perforation Penetrating ulcer
胃十二指肠溃疡急性穿孔Differential diagnosis 1.Hallmark of free perforation 2.Acute pancreatitis 3.Acute appentitis
Perforation Medical therapy: • > 24h, • Close surveillance.
溃疡病急性穿孔治疗 1.非手术治疗 适应证:症状轻、一般情况好的单纯性空腹 较小穿孔。 方法:胃肠减压、输液和抗生素等。 治疗6~8小时后,症状、体征加重者,改手术治疗。
溃疡病急性穿孔治疗 • 2.手术治疗 • 手术适应证:饱食后穿孔、顽性溃疡穿孔和伴有幽门梗阻、大出血、恶变等并发症者。
Perforation Operative approach: • Emergency closure (Oversewing)单纯穿孔缝合术, • Definitive ulcer operation。
Perforation • Operative approach: Emergency closure (Oversewing), Definitive operations. .
溃疡病急性穿孔治疗 • 3.手术方法 • 单纯穿孔缝合术:操作简便,危险性较少 • 彻底性手术。
溃疡病急性穿孔治疗 • 3. 手术方法 • 单纯穿孔缝合术; • 彻底性手术。
Gastric Outlet Obstruction • Surgery: reliefe of obstruction, antiulcer operation.
Gastric Outlet Obstruction • Fibrosis, scarring, deformity, (spasm,edema). • Gastric atony, gastric retention : bloating, anorexia, nausea, vomiting. • Endoscopic balloon dilatation+stent. • Surgery: absolute indication.
Peptic Ulcer HemorrhageBleeding Peptic Ulcer • 40 %- 60 % of all upper GI Hemorrhage • 6 %-15% in DU,2%-5% in GU • Conservative therapy, Endoscopy 80% • Surgical indication: Severe, persistent or recurrentbleeding; age, general health condition, other ulcercomplications. • Surgery is required in ca. 10% of patients
Self-limited: 80% • Mortality: 8% to 10% • resuscitation • endoscopy
Peptic Ulcer Hemorrhage 手术治疗 • 单纯缝合术; • 彻底性手术。
Postgastrectomy Syndromes • Postoperative Complications for Peptic Ulcer Disease
DUMPING SYNDROME • Dumping syndrome refers to a symptom complex that occurs following ingestion of a meal when a portion of the stomach has been removed or the normal pyloric sphincter mechanism has become disrupted.
DUMPING SYNDROME • Early Dumping syndrome :usually occurs within 20 to 30 minutes following ingestion of a meal; • Late Dumping syndrome:appears 2 to 3 hours after a meal
METABOLIC DISTURBANCES • Iron deficiency anemia • impairment in vitamin B12 metabolism:Megaloblastic anemia
EFFERENT LOOP OBSTRUCTION • The most common cause of efferent loop obstruction is herniation of the limb