Download
1 / 16
160 likes | 291 Views
Why discrepant evaluations manifest in ratings of QoL in dementia. Kritika Samsi, Vanessa Lawrence, Joanna Murray, Sube Banerjee PhD student, Mental Health & Ageing, Health Services & Population Research Department, Institute of Psychiatry Funded by: Guy’s and St Thomas’ Charitable Foundation.

E N D
Why discrepant evaluations manifest in ratings of QoL in dementia Kritika Samsi, Vanessa Lawrence, Joanna Murray, Sube Banerjee PhD student, Mental Health & Ageing, Health Services & Population Research Department, Institute of Psychiatry Funded by: Guy’s and St Thomas’ Charitable Foundation
Background • Dementia affects approx 24.3 million people worldwide; 4.6 million new cases every year • Interest in quality of life led to development of quantitative outcome measures • Discrepant evaluations between self-rated and carer-rated QoL commonly reported in studies of dementia • Reasons for this are speculated and implications investigated, mainly in terms of which account is superior and, therefore, more ‘reliable’ • Independent qualitative studies highlight variety of ways people with dementia and carers conceptualize QoL • Little integration of methods/studies to obtain a clearer understanding of discrepant evaluations in QoL and what it means
Study objectives • To measure relationship between self-rated and carer-rated QoL in dementia • To explore experience of QoL as perceived by people with dementia and their carers? • What influences the evaluations that people with dementia and carers make?
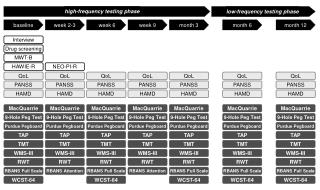
Research design • Mixed method study was designed as part of a larger study of change in QoL in dementia • Study 1: assessment of self-rated and carer-rated QoL and other clinical variables at 2 time points, 6 months apart • Correlation studies to determine consistency between perspectives • Study 2: qualitative study using Interpretative Phenomenological Analysis to gain in-depth understanding of experience of QoL • Interviews included experience of change, management of change • Ultimately to investigate the relationship between these 2 studies and integrate the findings from both studies to explicate the reasons for discrepant evaluations
Participants • Study 1: • @ BL people with dementia 121, carers 121 • @ FU people with dementia 77, carers 75 • No sig. differences between drop-outs and those retained • Study 2: • Homogenous purposive sample selected from Study 1 participants to reflect “information rich” cases • Participant characteristics • 9 people with dementia: 4 women, 5 men • 9 carers: 4 children, 5 spouses
Results from Study 1 • Statistically significant poor correlation between self-rated and carer-rated QoL on DEMQOL & DEMQOL Proxy and QOLAD & QOLAD Carer at both time points
Findings from Study 2 • People with dementia and carers described QoL in different ways • Carers reported on their relative or friend’s QoL in terms of their current health condition • Interviewer: To start with, can you tell me about your mother-in-law. • Edith (caring for her mother-in-law): What now? What she’s like now? Or what she was like? • Interviewer: As you wish. • Edith (caring for her mother-in-law): She is hard. She has lost her personality, but sometimes it comes back you know, like you will have, sort of a whole sentence, and it’s mum but then it goes and she has just become less and less communicative. She was a lovely person, she’s totally changed. • People with dementia focused on the positives and what they could still do • Ian (person with dementia): About me? Well, you know, I’m at a certain age, and, 88 I think, so I’m quite old and well, what can I say about that? I’ve enjoyed my life, I enjoy my life still but of course, I am limited because of my age, therefore I’m not so active and I can’t do things as I used to do.
Evaluation of changes • Three factors were found to be responsible for these discrepant evaluations: • Attributions of change • Management of change • Points of reference used for making evaluations
Attributions of change • Carers • Focused on lost abilities as a result of dementia • Sarah (caring for her mother): I lay her clothes out in order, and even now she might not put her petticoat on properly, its definitely that she’s not capable, she gets quite distressed with herself if she gets it wrong, so I lay out in order and try and make things simple. • People with dementia • Attribute changes to other conditions of “old age”, such as physical problems and social situations • Estelle (person with dementia): Well I used to work and so that has all stopped. But because of my health and my diabetes, there hasn’t been too much of a change if that’s what you mean. I’m still the same person, I still like doing what I’ve always liked and so there hasn’t been that much of a change.
Management of change : Carer • Carers managed changes by approaching caregiving in a practical proactive manner • This was by: • Seeking information • Support from services • Informal support • Practical coping styles • Jonathan (caring for his father): I have the overall, I am more or less running everything in the sense of making sure there is food here, making sure he’s got clean clothes on, making sure he is OK for everything, I accompany him to all of his appointments, chiropody, GP, ophthalmologist. I try and keep tabs on the (paid) carer, a (paid) carer comes in 3 times a day, I keep tabs on, so she is aware of what’s going on of course, make her aware of anything she needs to be aware of and try and keep the house in some sort of you know order. With the carers, you’ve probably heard before the complaints about them, I have to remind them sometimes about something. But generally they do the basic running of the house, if a plumber needs to be called, I control all his finances.
Management of change : Person with dementia • People with dementia managed changes by adapting psychologically to the situation • Their personal coping styles predominantly focused on having a positive attitude to their situation • Marion (person with dementia): Well my memory is not like it was. But not anything that upsets me, I remember when its mealtime. I think I’m pretty luck to have got to this age with so little physical problems, you know. I forget things, you know, bits of things, but I like to read.
Points of reference for making evaluations • Carers compared their relative or friend with dementia to what they used to be like in the past • Resulting in negative comparisons • Carol (caring for her husband): Its not bad but I mean in the old days he used to garden, now he never gardens, doesn’t do anything, nothing at all. He will come shopping with me and carry a few bits of shopping but that’s about all. He just hasn’t got the energy or the inclination anymore. • People with dementia, however, compared themselves to others in situations worse off than theirs • Resulting in positive comparisons • David (person with dementia): I would say it [quality of life] was good. I think when I see how hard it is for some people, of course I think its good, its good, I’m lucky, that’s what I say, lucky.
Attributions: Dementia Coping style: Practical proactive approach to caregiving Reference point: ‘Then & Now’ Attributions: “Old age” Coping style: Psychological, focusing on positives Reference point: Social comparisons Carer reported patient QoL Patient reported QoL
Implications • Methodological Implications • Self-rated and carer-rated QoL often investigated for reliability of account • Study 2 highlights the mechanisms by which evaluations are being made and that people with dementia and carers may be using different attributions of change • Different techniques to manage change may also influence responses • Both perspectives necessary in QoL assessments as they provide holistic view on quality of life • Service implications • Services for carers will ultimately benefit person with dementia due to carers’ practical approach to changing situation • Psychosocial interventions for people with dementia can sustain good QoL over time
Acknowledgements • Thank you to all participants who generously shared their views, specifically those who agreed to a third interview. • Thank you to Clare Flach, statistician (Institute of Psychiatry) for statistical advice. • Thank you to Rosalind Willis for assistance with data collection for Study 1.