Download
1 / 1
10 likes | 154 Views
bsl. w12. w24. fup. Demographics. fat mass in diff. areas. Sex . 15 male, 1 female. VAT [cm 2 ]. 121 ± 70. 78 ± 49. 68 ± 37. 94 ± 53. Age [years]. 44.8 ± 7.6. VAT/TAT-ratio. 0.39 ± 0.2. 0.34 ± 0.2. 0.33 ± 0.2. 0.36 ± 0.18. HIV and treatment history.

E N D
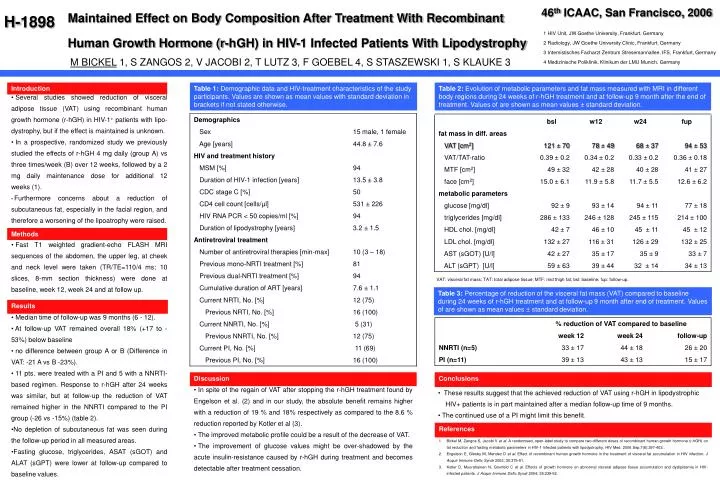
bsl w12 w24 fup Demographics fat mass in diff. areas Sex 15 male, 1 female VAT [cm2] 121 ± 70 78 ± 49 68 ± 37 94 ± 53 Age [years] 44.8 ± 7.6 VAT/TAT-ratio 0.39 ± 0.2 0.34 ± 0.2 0.33 ± 0.2 0.36 ± 0.18 HIV and treatment history MTF [cm2] 49 ± 32 42 ± 28 40 ± 28 41 ± 27 MSM [%] 94 face [cm2] 15.0 ± 6.1 11.9 ± 5.8 11.7 ± 5.5 12.6 ± 6.2 Duration of HIV-1 infection [years] 13.5 ± 3.8 metabolic parameters CDC stage C [%] 50 glucose [mg/dl] 92 ± 9 93 ± 14 94 ± 11 77 ± 18 CD4 cell count [cells/µl] 531 ± 226 triglycerides [mg/dl] 286 ± 133 246 ± 128 245 ± 115 214 ± 100 HIV RNA PCR < 50 copies/ml [%] 94 HDL chol. [mg/dl] 42 ± 7 46 ± 10 45 ± 11 45 ± 12 Duration of lipodystrophy [years] 3.2 ± 1.5 LDL chol. [mg/dl] 132 ± 27 116 ± 31 126 ± 29 132 ± 25 Antiretroviral treatment AST (sGOT) [U/l] 42 ± 27 35 ± 17 35 ± 9 33 ± 7 Number of antiretroviral therapies [min-max] 10 (3 – 18) ALT (sGPT) [U/l] 59 ± 63 39 ± 44 32 ± 14 34 ± 13 Previous mono-NRTI treatment [%] 81 Previous dual-NRTI treatment [%] 94 Cumulative duration of ART [years] 7.6 ± 1.1 Current NRTI, No. [%] 12 (75) Previous NRTI, No. [%] 16 (100) % reduction of VAT compared to baseline Current NNRTI, No. [%] 5 (31) week 24 follow-up week 12 Previous NNRTI, No. [%] 12 (75) NNRTI (n=5) 33 ± 17 44 ± 18 26 ± 20 Current PI, No. [%] 11 (69) PI (n=11) 39 ± 13 43 ± 13 15 ± 17 Previous PI, No. [%] 16 (100) 46thICAAC, San Francisco, 2006 Maintained Effect on Body Composition After Treatment With Recombinant Human Growth Hormone (r-hGH) in HIV-1 Infected Patients With Lipodystrophy H-1898 1 HIV Unit, JW Goethe University, Frankfurt, Germany 2 Radiology, JW Goethe University Clinic, Frankfurt, Germany 3 Internistisches Facharzt Zentrum Stresemannallee, IFS, Frankfurt, Germany 4 Medizinische Poliklinik, Klinikum der LMU Munich, Germany M BICKEL 1, S ZANGOS 2, V JACOBI 2, T LUTZ 3, F GOEBEL 4, S STASZEWSKI 1, S KLAUKE 3 Introduction Table 1: Demographic data and HIV-treatment characteristics of the study participants. Values are shown as mean values with standard deviation in brackets if not stated otherwise. Table 2: Evolution of metabolic parameters and fat mass measured with MRI in different body regions during 24 weeks of r-hGH treatment and at follow-up 9 month after the end of treatment. Values of are shown as mean values ± standard deviation. • Several studies showed reduction of visceraladipose tissue (VAT) using recombinant human growth hormone (r-hGH) in HIV-1+ patients with lipo-dystrophy, but if the effect is maintained isunknown. • In a prospective, randomized study we previously studied the effects of r-hGH 4 mg daily (group A) vs three times/week (B) over 12 weeks, followed by a 2 mg daily maintenance dose for additional 12weeks (1). • Furthermore concerns about a reduction of subcutaneous fat, especially in the facial region, and therefore a worsening of the lipoatrophy were raised. Methods • Fast T1 weighted gradient-echo FLASH MRI sequences of the abdomen, the upper leg, at cheek and neck level were taken (TR/TE=110/4 ms; 10 slices, 8-mm section thickness)were done at baseline, week 12, week 24 and at follow up. VAT: visceral fat mass; TAT: total adipose tissue; MTF: mid thigh fat; bsl: baseline; fup: follow-up. Table 3: Percentage of reduction of the visceral fat mass (VAT) compared to baseline during 24 weeks of r-hGH treatment and at follow-up 9 month after end of treatment. Values of are shown as mean values ± standard deviation. Results • Median time of follow-up was 9 months (6 - 12). • At follow-up VAT remained overall 18% (+17 to -53%) below baseline • no difference between group A or B (Difference in VAT: -21 A vs B -23%). • 11 pts. were treated with a PI and 5 with a NNRTI-based regimen. Response to r-hGH after 24 weeks was similar, but at follow-up the reduction of VAT remained higher in the NNRTI compared to the PI group (-26 vs -15%) (table 2). • No depletion of subcutaneous fat was seen during the follow-up period in all measured areas. • Fasting glucose, triglycerides, ASAT (sGOT) and ALAT (sGPT) were lower at follow-up compared to baseline values. Discussion Conclusions • In spite of the regain of VAT after stopping the r-hGH treatment found by Engelson et al. (2) and in our study, the absolute benefit remains higher with a reduction of 19 % and 18% respectively as compared to the 8.6 % reduction reported by Kotler et al (3). • The improved metabolic profile could be a result of the decrease of VAT. • The improvement of glucose values might be over-shadowed by the acute insulin-resistance caused by r-hGH during treatment and becomes detectable after treatment cessation. • These results suggest that the achieved reduction of VAT using r-hGH in lipodystrophic • HIV+ patients is in part maintained after a median follow-up time of 9 months. • The continued use of a PI might limit this benefit. References • Bickel M, Zangos S, Jacobi Vet al. A randomised, open-label study to compare two differentdoses of recombinant human growth hormone (r-hGH) on fat reduction and fasting metabolic parameters in HIV-1 infected patients with lipodystrophy. HIV Med. 2006 Sep;7(6):397-403.. • Engelson E, Glesby M, Mendez D et al.Effect of recombinant human growth hormone in the treatment of visceral fat accumulation in HIV infection. J Acquir Immune Defic Syndr 2002; 30:379-91. • Kotler D, Muurahainen N, Grunfeld C et al.Effects of growth hormone on abnormal visceral adipose tissue accumulation and dyslipidemia in HIV-infected patients. J Acquir Immune Defic Syndr 2004; 35:239-52.