Download
1 / 30
330 likes | 421 Views
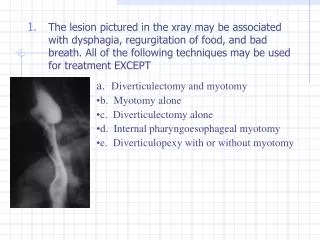
P.O.E.M. Per Oral Endoscopic Myotomy Procedure. McKenzie Quevillon BScN & Dawn Banavage RN. Background. Per Oral Endoscopic Myotomy Procedure. The lower esophageal sphincter (LES) is tight and stays closed during swallowing.

E N D
P.O.E.M. Per Oral Endoscopic Myotomy Procedure McKenzie Quevillon BScN & Dawn Banavage RN
Background Per Oral Endoscopic Myotomy Procedure • The lower esophageal sphincter (LES) is tight and stays closed during swallowing. • The esophagus is unable to move food into the stomach. This leads to the backup of food in the esophagus. • Why the esophageal muscles fail to relax in people with Achalasia is unknown. Researchers think there may be a link to a virus; and recent studies show that Achalasia may be an autoimmune disorder. • These patients also have an increased risk of esophageal cancer.
Achalasia Per Oral Endoscopic Myotomy Procedure
Endoscopic vs. Fluoroscopic Imagery Per Oral Endoscopic Myotomy Procedure
Current Treatments for Achalasia • Pneumatic dilation and laparoscopic Heller Myotomy. • Heller Myotomy: approach from outside of the stomach in through the cardia which involves dissecting all the of the tissue around the gastro esophageal junction (GEJ). • Botox injection is offered to patients that are not candidates for endoscopic or surgical approaches. This only offers temporary relief of symptoms.
Pneumatic Dilation Per Oral Endoscopic Myotomy Procedure
Botox Injection Per Oral Endoscopic Myotomy Procedure
What is P.O.E.M. ? Per Oral Endoscopic Myotomy Procedure • Per Oral Endoscopic Myotomy (P.O.E.M.) is a new procedure designed as an alternative to pneumatic dilation or laparoscopic Heller Myotomy, a larger, more invasive surgery. • Patients with Type I, II or III Achalasia could qualify for a P.O.E.M. • Safe and effective, minimally invasive technique used to treat Achalasia.
Who can have P.O.E.M. ? Per Oral Endoscopic Myotomy Procedure • Patients are evaluated both endoscopically and using manometry • With the use of high resolution manometry, achalasia is classified into Type I, II and III. • Type I is achalasia with minimal esophageal pressurization, • Type II is achalasia with esophageal compression • Type III is achalasia with esophageal spasm
Ling Classification Per Oral Endoscopic Myotomy Procedure • Two endoscopists (Li HK and Linghu EQ) independently recorded the characteristics of the middle and lower parts of the esophagus. • Includes three kinds of endoscopically viewed structures: multi-ring structure, crescent-like structure and diverticulum structure. • Three Types: • Type I – smooth without multi-ring, crescent-like structure or diverticulum structure. • Type II – with multi-ring or crescent-like structure but without diverticulum structure. • Type III – with diverticulum structure. Types II and III are further divided into subtypes.
According to the Ling Classification who can have P.O.E.M.? Per Oral Endoscopic Myotomy Procedure • Patients who are Type I are the most safe to do. • Patients who are Type IIa have also undergone successful P.O.E.M. with minimal difficulties, and some patients who fall into the Type IIb category can be considered on an individual basis. • More recently, patients that have type III may be P.O.E.M. candidates but would require a longer myotomy.
Eckardt Score • A tool to assess dysphagia • Patient is scored using this tool pre procedure and 3 months post P.O.E.M.
Method Per Oral Endoscopic Myotomy Procedure • Procedure is done under a general anesthesia, and takes approximately 2 hours. • Endoscope is passed to evaluate GEJ. • Measurements are taken to determine length of myotomy. • An incision is made in the esophageal mucosa with an instrument that injects and cuts. This technique is used to tunnel between the mucosa and the muscle to just beyond the GEJ. • The myotomy is then done where the circular muscle layer is cut. • Mucosal incision is closed with multiple endoclips.
Submucosal Tunneling Per Oral Endoscopic Myotomy Procedure
Mucosal Closure with Endoclips Per Oral Endoscopic Myotomy Procedure
Adverse Events Per Oral Endoscopic Myotomy Procedure • Insufflation-related: pneumoperitonium, pneumomediastinum and subcutaneous emphysema • Bleeding: minor intraprocedural bleeding is common and managed by using a coagulation grasper. Post procedure bleeding incidence reports to be 1.1%. • Mucosal Perforation: repaired endoscopically • GERD and/or Erosive Esophagitis ranged from 11-19%
Nursing Measures Pre-Procedure • Baseline measurement of neck circumference • Endo-Pause (Time-Out) • Patient assessment • History • Assist Anesthesia with intubation
Nursing Measures Intraprocedurally Per Oral Endoscopic Myotomy Procedure • Ensure Anesthesia is aware to monitor for an increase in the patients peak airway pressures and ETCO2. • Subcutaneous air, pneumoperitoneum, pneumomediastinum are risks which would be evidenced by increases in peak airway pressures. • Assessment for crepitation’s in neck and chest through palpation. • Assessment of abdomen for abdominal distention with tension through palpation and visual inspection as patients are lying supine for procedure.
What do you do if the patient has abdominal distension with tension? Per Oral Endoscopic Myotomy Procedure Placement of Verres Needle The umbilicus is the ideal site of choice for insertion: • The thinnest area • Minimal subcutaneous fat
Post Procedure Assessments Per Oral Endoscopic Myotomy Procedure Crepitus: During our first P.O.E.M. cases patients did have some crepitus in the neck palpated intra procedurally and post procedure. This should resolve but, if this does not or you palpate more crepitus ask physician to assess patient. Measurement tool in place to measure the degree of subcutaneous air. Bleeding: This would be categorized by hematemesis or decreased hemoglobin. The patient should be assessed by physician and may need to have repeat endoscopy.
Post Procedure Care Per Oral Endoscopic Myotomy Procedure • Patient is kept nothing by mouth (NPO) until after the repeat endoscopy is done. • Endoscopy done the following day to assess mucosal closure (clips intact) and for any adverse events such as bleeding. • Barium swallow done at physicians discretion. • Pain management using opioids, acetaminophen and nonsteroidal anti-inflammatory drugs. Most patients in our experience have not experienced any significant pain post procedure.
Discharge and Follow-up • Strict diet post procedure to ensure optimal healing • 24 hours post procedure: clear liquids • 48 hours post and up to 2 weeks: full fluids and then advanced to soft diet avoiding alcohol, crunchy, spicy or foods you need to chew a lot. • After one week: return to normal diet. • 3 month follow-up endoscopy to assess for symptoms of dysphagia, esophagitis and a repeat Eckardt score.
What about the endoclips? Per Oral Endoscopic Myotomy Procedure • The endoclips used are “MRI Conditional”, meaning the patient should be able to have an MRI done with the endoclips in place. • This being said, if your patient is to have an MRI, please inform MRI staff that the endoclips are in place, just so that they are made aware.
Results Per Oral Endoscopic Myotomy Procedure • Enables shorter hospital stay, faster recovery. • Patients are being discharged in 2-4 days and are reporting an almost immediate improvement in swallowing. • Facilitating positive patient outcomes by educating staff on post procedure care of patients on floor. • The procedure is effective in >90% of achalasia patients, and the rate of serious adverse events is generally <5%.
P.O.E.M. Video from St Michael’s Hospital Per Oral Endoscopic Myotomy Procedure
Nursing Initiatives • General Anesthesia training • Proper patient positioning • Training in animal lab • Cautery Training/Certification • ACLS trained nurses with critical care experience • Training for surgical floor nurses on post procedure care • Creation of PIC lists
References Per Oral Endoscopic Myotomy Procedure Bechara, R., ikeda, H., & Inoue, H.. (2015). Peroral endoscopic myotomy:an evolving treatment for achalasia. Nature Reviews gastroenterology & Hepatology, 12: 410-426. Li, H., & Linghu, E.. (2013). New endoscopic classification of achalasia for selection of candidates for peroral endoscopic myotomy. World Journal of Gastroenterology, 19(4): 556-560. Misra, L., Fukami, N., Nikolic, K & Trentman, T.. (2017). Peroral endoscopic myotomy: procedural complications and pain management for the perioperative clinician. Med Devices, 10: 53-59. Pannala, R., Dayyeh,B., Aslanian, H., Enestvedt, B., Komanduri, S., Manfredi, M., Maple, J., Navaneethan, U., . Parsi, M., Smith, Z., Sullivan, S., Thosani, N., & Banerjee, S.. (2016). Per-oral endoscopic myotomy. ASGE, 83(6). Stoltzfus, S. & Boskey, E.. (2015). Achalasia: causes, symptoms & diagnosis. Healthline.