Download
1 / 33
340 likes | 346 Views
Parkinson's Disease. ILOs At the end of this lecture you will be able to:- Recognize the symptoms and pathophysiology of parkinsonism. Understand the pharmacology of drugs used for treatment of parkinsonism. Quiz?. Neurological presentations of Parkinsonism EXCEPT: A- rigidity

E N D
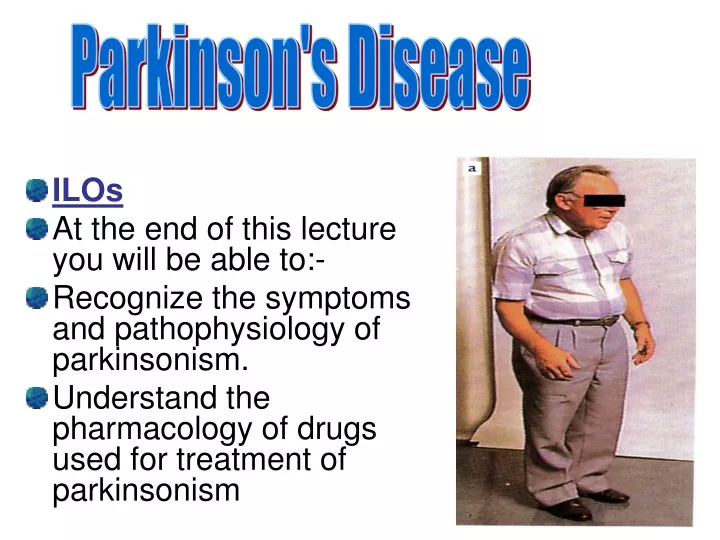
Parkinson's Disease • ILOs • At the end of this lecture you will be able to:- • Recognize the symptoms and pathophysiology of parkinsonism. • Understand the pharmacology of drugs used for treatment of parkinsonism
Quiz? • Neurological presentations of Parkinsonism EXCEPT: A- rigidity B- hyperkinesia C- tremor D- postural disturbances. E- poor balance
Drug Treatment • Replacement of dopamine by levodopa. • Levodopa is used with dopa decarboxylase inhibitors e.g. carbidopa , benserazide • or COMT inhibitor e.g. entacapone.
Drugs that mimic the effects of dopamine at D2 & D3-receptors e.g. bromocriptine, pramipexole and ropinirole. • MAO-B inhibitors e.g. selegiline • Drugs that release dopamine e.g. amantadine • Muscarinic acetylcholine antagonists e.g. benzatropine, trihexphenidyl and procyclidine.
Levodopa • First –line treatment , combined with peripheral dopa decarboxylase inhibitor. • Absorbed from the small intestine by active transport, t½=2h • All types of parkinsonism except those associated with antipsychotic drug therapy.
Wearing-off effect. • On-off effect. • →progression of the disease and the loss of striatal dopamine nerve terminals. • dyskinesias. [Occur in 40 to 90% of patients]. • → fluctuating plasma levels of levodopa and the presence of hypersensitive dopamine receptors. • The dyskinesias can be reduced by lowering the dosage; however, the symptoms of parkinsonism may then reappear.
ADRs:- • Peripheral side effects are anorexia, nausea, and vomiting (due to stimulation of the CTZ). • Orthostatic hypotension ,Cardiac arrhythmias occur in some patients. • CNS adverse effects of levodopa therapy include vivid dreams, delusions, hallucinations, confusion and sleep disturbances.
Interactions:- • Proteins ingested with meals. • Nonselective MAO inhibitors (phenelzine, tranylcypromine). • Pharmacologic doses of pyridoxine.
Contrindications • Psychotic patient. • Angle closure glaucoma. • With caution to patients with active ulcer. • Patients with history of melanoma.
Quiz? • Carbidopa is useful in treatment of Parkinson’s disease because:- (A) Is a precursor of levodopa (B) Is a dopamine receptor agonist (C) Prevents peripheral biotransformation of L-dopa (D) Prevents a breakdown of dopamine (E) Promotes a decreased concentration of L-dopa in the nigrostriatum
Dopamine receptor agonists • long duration of action , less likely to cause dyskinesias than levodopa. • As monotherapy, the dopamine agonists are less effective than levodopa.
When used as an adjunct to levodopa in advanced stages, they may contribute to clinical improvement and reduce levodopa dosage needs. • Example ,bromocriptine.
Bromocriptine • Bromocriptine, an ergot derivative, is an agonist at the D2-receptors and a partial D1-antagonist. • Bromocriptine is absorbed to a variable extent from the GIT ; peak plasma levels are reached within 1–2 hours after an oral dose.
It is excreted in the bile and feces. • ADRs:- • Postural hypotension, nausea, somnolence • Dyskinesias. • Confusion, hallucinations, delusions, • In order to minimize adverse effects, the dose is built up slowly over 2 or 3 months. • Used for hyperprolactinemia.
Contraindications • In patients with a history of psychotic illness . • Recent myocardial infarction, • Active peptic ulceration. • The ergot-derived dopamine agonists are best avoided in patients with peripheral vascular disease.
Quiz? • Which one of the following statements about bromocriptine is accurate? (A) It should not be administered to patients taking antimuscarinic drugs (B) Effectiveness in Parkinson's disease requires its metabolic conversion to an active metabolite (C) The drug is contraindicated in patients with a history of psychosis (D) The drug should not be administered to patients already taking levodopa (E) Mental disturbances occur more commonly with levodopa than with bromocriptine.
Amantadine • originally introduced as an antiviral. • modestly effective in treating symptoms of parkinsonism. • Useful in the early stages of parkinsonism or as an adjunct to levodopa therapy.
Amantadine affects dopamine release and reuptake. • antagonist at muscarinic and NMDA receptors. • Peak plasma concentrations of are reached 1–4 hours after an oral dose. • t½=2-4h, most of the drug being excreted unchanged in the urine.
Adverse effects include:- • nausea, dizziness, insomnia, confusion, hallucinations, • ankle edema, and livedo reticularis. • Amantadine and the anticholinergics may exert additive effects on mental functioning. • Should be used with caution in patients with a history of seizures or heart failure.
Selegiline is an irreversible inhibitor of MAO-B, an important enzyme in the metabolism of dopamine. • Blockade of dopamine metabolism makes more dopamine available for stimulation of its receptors.
Selegiline, as monotherapy, may be effective in the newly diagnosed patient with parkinsonism. • It enhances the actions of endogenous dopamine.
Selegiline is also used in conjunction with levodopa–carbidopa in later-stage parkinsonism to:- • reduce levodopa dosage requirements • and to minimize or delay the onset of dyskinesias and motor fluctuations that usually accompany long-term treatment with levodopa.
Selegiline may slow the progression of the disease by reducing the formation of toxic free radicals produced during the metabolism of dopamine. • Metabolized to desmethylselegiline, Which is antiapoptotic.
ADR:-at higher doses Selegiline may inhibit MAO-A. • Selegiline may cause insomnia when taken later during the day. • The adverse effects of levodopa may be increased by selegiline. • Selegiline should not be coadministered with TCA, meperidine or SSRIs. (may cause hyperpyrexia, agitation, delirium, coma).
Anticholinergic Drugs • The efficacy of anticholinergic drugs in parkinsonism is due to their ability to block muscarinic receptors in the striatum. • They exert only modest antiparkinsonian actions , used during the early stages of the disease or as an adjunct to levodopa therapy. • Anticholinergics can provide benefit in drug- induced parkinsonism. • e.g. Benztropine, Trihexyphenidyl.
ADR- cycloplegia, dry mouth, urinary retention, and constipation. • Confusion, delirium, and hallucinations may occur at higher doses. • Trihexyphenidyl may cause withdrawal symptoms in patients receiving large doses.
Quiz? • Great caution must be exercised in the use of this drug in parkinsonian patients who have prostatic hypertrophy or obstructive gastrointestinal disease:- • (A) Benztropine • (B) Carbidopa • (C) Levodopa • (D) Ropinirole • (E) Selegiline
Quiz? • A drug that is used in the treatment of parkinsonism and will also attenuate reversible extrapyramidal side effects of neuroleptics is • (A) Amantadine • (B) Levodopa • (C) Pergolide • (D) Selegiline • (E) Trihexyphenidyl