Download
1 / 27
280 likes | 397 Views
“It’s all in your head”. Kyle McLaughlin Sept. 1, 2005 Diagnostic Imaging Rounds. Case of R.M. 28 M, 3 mos Hx of Headache Headache: diffuse, constant, 4-10/10 No previous Hx of H/A Tx for HTN and migraine with no success Booked for H/A clinic by Family MD. Case of R.M.

E N D
“It’s all in your head” Kyle McLaughlin Sept. 1, 2005 Diagnostic Imaging Rounds
Case of R.M. • 28 M, 3 mos Hx of Headache • Headache: diffuse, constant, 4-10/10 • No previous Hx of H/A • Tx for HTN and migraine with no success • Booked for H/A clinic by Family MD
Case of R.M. • What else do you want to know?
H/A worse with lying down, late at night and early a.m. Assoc. Sx Nausea Dizziness Vague diplopia Word finding difficulties Mild personality change PMHx- healthy Meds- none, NKDA FHx- unremarkable P/E: Unremarkable except poor R sided Upper Extremity Cerebellar testing Case of R.M.
What next? • DDx? • Investigations? • Imaging? • Why?
What now? • DDx? • Disposition and Management?
Case of R.M. • Diagnostic Imaging: • CT head- Dx with astocytoma • MRI- low grade glioma
Case of R.M. • Transferred to Neurosurgery, started on Dexamethasone • Craniotomy for excision of brain tumour 3 days later • Negative culture • Biopsy result: primitive neuroepithelial tumour
Headaches and Brain Tumours • Headache present in 50-60% of brain tumours • Pain secondary to: • Vessel traction, distention and dilation • Direct pressure on CN with pain afferents • Inflammation around pain sensitive structures (venous sinuses, portion of the dura, dural arteries, cerebral arteries)
Headache Red Flags • New or changed • Exertional • Onset at night or early a.m. • Progressive in nature • Fever or systemic Sx • Meningismus • Neuro Sx • Valsalva maneuver worsens • Age: New onset >50 y.o. or in children
Conditions to Rule Out • Space occupying lesion • Meningitis, encephalitis • Stroke • Subarachnoid hemorrhage • Systemic illness (thyroid, HTN, pheochromocytoma, etc.) • Temporal arteritis • Traumatic head injuries • Serious ophthalmologic and otolaryngologic etiology Purdy, A., Kirby, S. Headaches and brain tumours. Neuro Clin Am 22 (2004) 39-53.
DDx of brain lesion • Tumour • Pus • Blood
Tumour • Adults • Infratentorial: • Mets (20-30%) • Schwannoma (6%) • Supratentorial: • Astrocytoma (40-50%) • Mets (20-30%) • Meningioma (15%) • Oligodendroglioma (5%)
Pus • Brain abscess • Local spread (i.e. OM, mastoiditis, sinusitis) • Hematogenous spread (i.e. immunosuppressed, lung abscess, empyema) • Dural disruption • Granuloma (TB, sarcoid)
Blood • Hematoma/hemorrhage • Epidural, subdural, SAH, etc. • Vascular Abnormality • Aneurysm, AV malformation • Ischemic cerebral infarction
Indications for imaging in headache • Sudden onset of “worst h/a of life” • New h/a in HIV + • A h/a that: • Worsens with exertion • Assoc with decreased alertness or mental status change • Awakens from sleep • Changes in pattern over time • Assoc with papilledema • Assoc with focal neurological deficit Mettler: Essentials of Radiology, 2nd ed, 2005
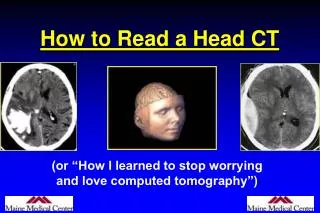
Imaging choices • CT • More accessible, quicker • Good initial scan in ruling out many etiologies (i.e.hemorrhage) • MRI • Superior soft tissue contrast • Good for further differentiation of: • Brain tumour • Undiagnosed intracranial lesions