Download
1 / 37
390 likes | 427 Views
Body Major Electrolytes. Positive Electrolytes assistant teacher Mohammed Abdullah Ahmed. The Body Compartments. The electrolyte concentration will vary with a compartment. The three body fluid compartments are; 1. Intracellular fluid (45-50%) of body weight.

E N D
Body Major Electrolytes Positive Electrolytes assistant teacher Mohammed Abdullah Ahmed
The Body Compartments The electrolyte concentration will vary with a compartment. The three body fluid compartments are; 1. Intracellular fluid (45-50%) of body weight. 2. Extracellular fluid, made of two parts; A) Interstitial fluid (12-15%) of body weight. B) Vascular fluid or plasma ( 4-5%) of body weight. The three compartments are separated from each other by permeable membranes. The later allows the passage of water and some inorganic as well as organic substances.
Units of Concentration Electrolyte concentrations are expressed by units N=gm/Eq.wt * 1/L N=mg/Eq.wt*1/L M=gm/M.wt* 1/L
Ex2: What is the weight of CaCl2 .2H2O needed to Ca+2/l? prepare a liter of solution containing 9mEq? Ex3: What will be the chloride content of a solution containing 661.5 mg CaCl2 .2H2O?
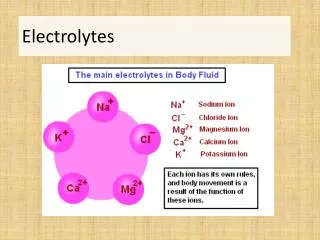
SODIUM Sodium is the principal cation in extracellular fluid. Its responsible for maintaining osmotic pressure and hydration. Its absorbed from daily diet by the intestinal tract. Excess sodium is excreted by the kidneys, The concentration of sodium is 142mEq/l in extracellular fluid, and 10 mEq/l in intracellular fluid.
Hyponatremia Conditions causing hyponatremia include: 1. Extreme urine loss such as seen in diabetes insipidus which caused by deficient insulin secretion by the beta cells of the islets of Langerans in the pancreas. 2. Metabolic acidosis, in which sodium is excreted. 3. Addison’s disease with decreased excretion of ADH. 4. Diarrhea and vomiting 5. Kidney damage
Hypernatremia Hypernateria may be caused by: 1. Cushing’s syndrome with increase in ADH production, 2. Severe dehydration, 3. Certain types of brain injury, 4. Excess treatment with sodium salts.
Sodium level and Hypertension Sometimes the body is unable to eliminate sodium and the concentration starts to increase, water is retained in the tissues to maintain osmotic balance, Edema results and the patient can take a puffy appearance with swelling, particularly of the lower extremities. The buildup of fluids puts an added burden on the heart which may be aggravated if the heart is also diseased. Treatment includes low salt diets, diuretics, cardiotonic drugs or combination of these.
Sodium Control and Replacement Sodium – free salt substitutes can be used to enhance the flavor of food. A wide vriety of these are now available in the market. Sodium Chloride: Oral 1 gram three times a day or IV 1 liter of a 0.9% solution. Fructose and sodium chloride injections; 10% fructose and 0.9% NaCl. It is nutrient and electrolyte replenisher.
POTASSIUM Potassium is the major intracellular cation present in concentrations approximately 23 times higher than the concentration of potassium in the extracellular fluid. The small fraction 2% of total body potassium which is in the extracellular fluid is distributed proportionately between the interstitial and the plasma. The concentration in serum is around 4.5mmol/l. The concentration content is maintained by an active transport mechanism. During transmission of a nerve impulse, potassium leaves the cell and sodium enters the cell, sodium-potassium pump.
Potassium Potassium in the diet is rapidly absorbed and the excess potassium is rapidly excreted by the kidneys. Potassium salts have been used for their diuretic action because of the efficient excretion of potassium by the kidneys, since a certain volume of urine will be excreted in order to keep the potassium salt in solution. Whole body counts of potassium can be found by measuring levels of potassium .
Hypopotassemia Hypopotassemia can be serious to the patient. It causes changes ECG and in myocardial function, flaccid and feeble muscles and low blood pressure. The main causes of hypopotassemia are; 1. Vomiting and Diarrhea 3. Burns 4. Hemorrhage 5. Diabetic coma 6. IV infusion of solution lacking in potassium 7. Overuse of diuretics 8. Alkalosis, movement of potassium into cells as protons move out of the cell into the proton deficient extracellular fluid.
Hyperpotassemia Hyperpotassemia is less common and occurs during certain types of kidney damage. If the kidney is functioning properly the body can eliminate excess potassium readily. In certain acidosis conditions, interference the sodium and potassium proton exchange can result in potassium retention. Potassium may be released from some damaged cells leading to increases serum potassium. Potassium Replacement 1. Potassium chloride, irritant to gastrointestinal tract. 2. Potassium Gluconate, less irritating than the chloride.
Potassium Level and the Heart The heart is sensitive to potassium concentrations. In hypopotassemia there are alterations in the ECG (fattened T wave) and disticthitological alterations in the myocardium. Hyperpotassimea also results in changes in the ECG (peaked T wave) and causes the heart muscles to become flaccid with possible cessation of heart beat (potassium unrest). It is thought that potassium may replace calcium in the cardiac muscle. Hyperpotassemia may be caused by kidney damage and acidosis.
CALCIUM About 99% of body calcium is found in bones and the remaining is present in extracellular fluid compartment. Only 10% of the ingested calcium is absorbed from the intestinal tract and the remainder is excreted with faeces. The concentration of calcium in plasma averages about 9.4mg/dl, (9-10mg/dl). calcium level in plasma is regulated within narrow limits by parathyroid hormone.
The calcium in plasma is present in three forms 1. About 40% is combined with plasma proteins and is non diffusible through the capillary membrane. 2. About 10% is combined with other substances of plasma and interstitial fluid (citrate, phosphate for instance) and is diffusible through the capillary membrane in such a manner that it is not ionized.
calcium The remaining 50% calcium present in plasma is diffusible through the capillary membrane and ionized. this ionic calcium does most of the functions of calcium in the body.
Calcium is important for: 1. blood clotting 2.contraction of smooth muscles. 3. In cardiovascular system (CVS) Calcium is essential for contraction coupling in cardiac muscles as well as for the conduction of electric impulse in certain regions of heart. 4.Calcium also plays role in maintaining the integrity of mucosal membrane, cell adhesion and function of the cell membrane as well
Hypocalcemia Hypocalcemia occurs due to: 1.hypoparathyroidism. 2.vitamin D deficiency. 3.Osteoblastic metastasis. 4.steatorrhea (fatty stools). 5. Cushing syndrome (hyperactive adrenal cortex). 6. acute pancreatitis and acute hyperphosphatemia.
Causes of Hypercalcemia Hypercalcemia is found in; 1. Hyperparathyroidism 2. Hypervitaminosis D. 3. Bone neoplastic disease 4. Diuretic therapy. 5. Immobilization: especially in young people or patients with Paget’s disease. 6. Milk alkali syndrome: the combination of increased calcium intake together with bicarbonate.
Calcium Replacement Calcium Replacement: 1. Calcium chloride contains 0.033% CaCl2 .2H2O 2. Calcium gluconate
Magnesium Magnesium is the second most plentiful cation in the intracellular fluid. About 50% of total body magnesium is combined with calcium and phosphates in bones. Essential component of many enzymes involving phosphate metabolism. Also used in functioning of neuromuscular system.
hypomagnesia Causes of hypomagnesia include: • Low intake of Mg in the diet. • Prolonged diarrhea Chronic alcoholism Gastrointestinal diseases Massive diuresis. hypoparathyroidism
Hypermagnesemia -Renal insufficiency- -dehydration. -Excessive use of Mg- containing antiacids or laxatives. Magnesium Replacement: Magnesium Sulphate, when injected used as Central nervous system (CNS) depressant, 4 grams in 10% solution. Magnesium sulphate; Oral dose 1-10 grams daily.
Chloride Chloride major extracellular anion is principally responsible for maintaining proper hydration, osmotic pressure, and normal cation anion balance in vascular and interstitial compartment. The concentration of chloride is 103mEq/l in extracellular fluid, and 4 mEq/l in intracellular fluid. Chloride ion has no pharmacological activity ,used as a urinary acidifier.
Hypochloremia Hypochloremia can be caused by; 1.salt losing nephritis, leading to lack of tubular reabsorption of chloride. 2. metabolic acidosis such as found in diabetes mellitus, 3. in renal failure 4.prolonged vomiting.
Hyperchloremia Hyperchloremia can be caused by; Dehydration decreased renal blood flow found with congestive heart failure. severe renal damage excessive chloride intake.
PHOSPHATE -Phosphate is the principal anion of intracellular fluid compartment. - Inorganic phosphate in the plasma is mainly in two forms HPO4-- and H2PO4- ,the concentration of HPO4-- is 1.05 mmole/L and the concentration of H2PO4- 0.26 mmole/L. - Important acid-base buffer in body fluids
PHOSPHATE When pH of the extracellular fluid becomes more acidic there is relative increase in H2PO4- and decrease in HPO4- - and vice versa. Phosphorous is essential for: 1. proper metabolism of calcium, 2. normal bone and tooth development. 3.HPO4-- and H2PO4- makes an important buffer system of body.
PHOSPHATE The main phosphate ion in intracellular fluid compartment is HPO4-2 Its main role can be summerised a follows: 1. ATP is the potential chemical energy storage which contains the phosphoric acid anhydride linkage. 2. The phosphate is important in the buffer system HPO4-2/ H2PO4- 3. The sugars hexoses are metabolized as phosphate esters.
PHOSPHATE Hyperphosphatemia can be found in: hypervitaminosisD. renal failure. hypoparathyoidism. Hypophosphatemia can be due to : vitamin D deficiency, hyperparathoidism. and possible long term aluminum hydroxide antacid therapy.