Download
1 / 5
50 likes | 283 Views
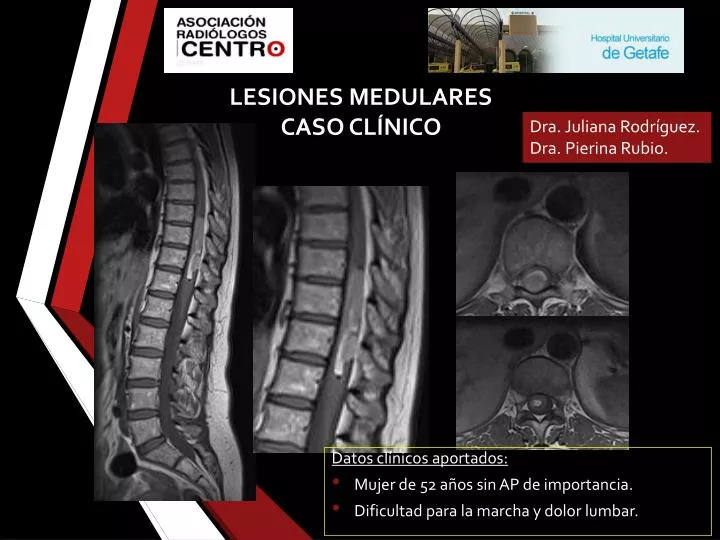
LESIONES MEDULARES CASO CLÍNICO. Dra. Juliana Rodríguez. Dra. Pierina Rubio. Datos clínicos aportados: Mujer de 52 años sin AP de importancia. Dificultad para la marcha y dolor lumbar. SAGITAL SE T1 SIN Y POST GD. SAGITAL Y AXIAL SE T2 CON FS.

E N D
LESIONES MEDULARESCASO CLÍNICO Dra. Juliana Rodríguez. Dra. Pierina Rubio. Datos clínicos aportados: • Mujer de 52 años sin AP de importancia. • Dificultad para la marcha y dolor lumbar.
SAGITAL SE T1 SIN Y POST GD SAGITAL Y AXIAL SE T2 CON FS 1. Cuál de los siguientes enunciados cree que es el más correcto? • Es una lesión de origen tumoral. • Es una lesión de origen inflamatorio. • Es una lesión vascular. • Ninguna de las anteriores.
Tumoral vs No tumoral El criterio de imagen esencial para un tumor intramedular es la expansión del cordón. La mayoría de los tumores muestran algún realce tras la administración de contraste. La presencia de quistes (tumorales y no tumorales) y siringohidromielia es un hallazgo comúnmente asociado a tumores intramedulares. 2. ¿ Como describiría la lesión? Intraduralextramedular. Intradural intramedular. Extraduralextramedular . Neoplasms of the Spinal Cord and FilumTerminale: Radiologic-PathologicCorrelation. RadioGraphics 2000; 20:1721–1749
3. ¿Cual es su diagnóstico? Duramadre INTRADURAL INTRAMEDULAR EXTRADURAL EXTRAMEDULAR INTRADURAL EXTRAMEDULAR • Neurofibroma • Melanoma • Meningioma • Astrocitoma
ASTROCITOMA • Segundo en frecuencia en adultos. • Tórax > cervical. • Mayoría de bajo grado (I o II). • RM : Masa excéntrica • Carácter infiltrativo • Márgenes peor definidos. • Hipo o iso en T1 e hiper en T2. • Realce irregular y parchead • Hemorragia infrecuente, no “capsign” • Ependimoma • Astrocitoma • Ganglioglioma • Hemagioblastoma • Metástasis • Linfoma • Melanoma • Tumores de la vaina nerviosa: Neurofibroma / Schwannoma • Meningioma • Paraganglioma • Lipoma • Hemangioma • Linfoma DDx lesiones intramedulares hiperintensas en T1. Generalmente la hiperintensidad en T1 puede deberse a hemorragia, grasa o melanina MELANOMA • Primario: Muy raro, 1 % de todos los melanomas. • > Torácico, edad media, ambos sexos. • Hiper T1, Iso o hipo en T2, realce moderado y homogéneo. • Frecuente hemorragia signo del anillo de hemosiderina o “capsign” . • En RM primario similar a metastásico.