Download
1 / 26
260 likes | 556 Views
Chagas Disease in the United States. FDA BPAC meeting, 1 April 2009. Susan P. Montgomery, DVM MPH LCDR, USPHS Parasitic Diseases Branch Centers for Disease Control and Prevention Atlanta, GA. Trypanosoma cruzi. Protozoan parasite only found in the Americas, causes Chagas disease

E N D
Chagas Disease in the United States FDA BPAC meeting, 1 April 2009 Susan P. Montgomery, DVM MPH LCDR, USPHS Parasitic Diseases Branch Centers for Disease Control and Prevention Atlanta, GA
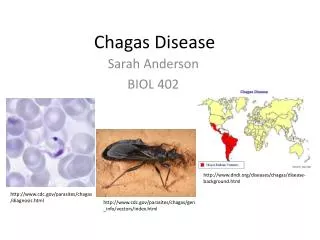
Trypanosoma cruzi • Protozoan parasite only found in the Americas, causes Chagas disease • Vector-borne zoonosis, humans not necessary to cycle • Infects >100 domestic and wild mammals • Typical hosts: opossums, wood rats, raccoons, dogs, cats • Infection of host and vector is life-long • Enormous domestic and sylvatic reservoirs
Distribution of vectors and disease • Endemic for human Chagas disease • Infected vectors, nonhuman mammals
Chagas disease worldwide • Programs in Latin America focus on controlling transmission • Vector control • Blood safety • WHO Global Network for Chagas disease formed in 2007 • Drug donation (nifurtimox) to WHO • Unique situation in the U.S.
Acute phase of Chagas disease T. cruzi infection 4 - 8 weeks Asymptomatic: > 90% Symptomatic: <10% Infection remains life-long if untreated Chronic phase Indeterminate form (asymptomatic, normal H&P, ECG) 20 - 40% progress over years - decades 60 - 80% remain in indeterminate form throughout life Can reactivate if immunosuppressed Clinically manifest Chagas disease Chagas heart disease Chagas gastrointestinal disease
Clinical testing challenges • No gold standard test for diagnosis • Serological testing limited availability and varied sensitivity and specificity • Specific skill necessary for parasitological diagnosis (acute infection, reactivation disease) • No test to identify which patients will progress from indeterminate form to clinical disease • No test to determine cure with antiparasitic treatment
Risk of infection in the U.S. • Estimated 300,000 infected immigrants in U.S.* • Who is at risk of infection in the U.S. • People exposed to infected vectors and/ or reservoirs • Children of infected mothers • Transplant recipients • Transfusion recipients • Laboratory staff working with vectors, reservoir species, or parasite *Bern and Montgomery, manuscript submitted
History of bugs and T. cruziin the United States • 1855 – Vector bugs identified in Georgia • 1860’s / 70’s – Vector bugs identified in six more states • 1909 – Discovery of parasite and disease (Brazil) • 1916 – Parasite first observed in California • 1930’s – Reservoir host infections studied in U.S. • 1955 – First autochthonous cases of Chagas disease reported
States with documentedpotential T. cruzi vectors ~ 11 potential vector species in the U.S.
States with documented mammalian reservoirs * * * * * Published human vector-associated cases > 18 infected reservoir species identified
30 mm Vector and Chagas disease in Texas* Overall, 50% of tested bugs positive for T. cruzi Female Triatoma gerstaekeri Male Triatoma sanguisuga *Kjos et al. VBZD 2009 Photo courtesy of Sonia Kjos
Vector-borne transmissionin the U.S. • Seven autochthonous human cases published
Published U.S. autochthonous cases:Acute infections • Age range 2 weeks to 84 years, 4 male • 4 presented with acute symptoms • Non-specific febrile illness • Myocarditis, pericardial effusion • 2 primary complaint of bug bites • Fever within 48 hours of bug identification • 1 unclear clinical history • Triatomines on property in 5 cases; infected reservoir animals on property in 4 cases
Autochthonous infections in U.S. blood donors • 2007 Investigation of two blood donors in Mississippi • Ongoing study to investigate potentially autochthonous cases, U.S.– Derived T. cruzi Infection Study (USTC) • Designed in collaboration with American Red Cross and Blood Systems Laboratories • Participants will be tested with blood center and CDC tests
Travel-associated infection • 26yo Canadian woman returned from 6 months in rural Mexico with acute Chagas disease (Romana’s sign) • 56yo Californian man asymptomatic positive blood donor, three international trips each < 2 wks • Two trips to Mexico, one to non-endemic area of South America
Congenital transmission in the U.S. • No confirmed cases in U.S. • 3 possible cases reported • Case reports from other non-endemic areas • Congenital transmission 1 – 10% in endemic areas • Usually asymptomatic or non-specific findings • Low birth weight, hepatosplenogmegaly, respiratory distress, anemia, fever • Estimate 63 – 315 infected infants per year in U.S.* *Bern and Montgomery, manuscript submitted
Transplant transmission in the U.S. • Five published cases • 24 recipients of solid organs from seropositive donors in U.S. • Heart • Liver • Kidney • Pancreas/ kidney, liver/ kidney, pancreatic islet • 7 (41 %) of 19 recipients became infected
Transfusion transmission in the U.S. and Canada • 7 transfusion transmission cases reported in U.S. and Canada • Likely under-recognized and under-reported
Laboratory-associated transmission in the U.S. • Possible exposures • Feces of infected triatomenes • Handling cultures from infected persons or animals • Routes of entry • Needlesticks • Existing micro-abrasions on skin • Mucus membranes • Inhaling aerosolized organisms? • 8 cases reported in the U.S. • 3 needlesticks • 3 contact with infectious material and break in skin • 2 unknown
Chagas disease may not be recognized in the U.S. • Most physicians not familiar with Chagas disease • Recent ACOG survey • Medscape surveys • Community-based organization focus groups • Even clinical Chagas disease is not diagnosed • Up to 14% of Hispanic cardiac patients found to be positive for Chagas disease (screened for typical EKG changes)
U.S. public health and Chagas disease • Not nationally notifiable • Reportable only in AZ, soon in MA • No systematic public health surveillance • AABB Biovigilance system • Competing priorities at public health departments • Lack of public health testing capacity for Chagas disease
2007 – 2008 CDC consultations and drug releases for Chagas-positive blood donors 45 drug releases 115 consultations (19 suspected autochthonous infections) Total of 765 RIPA-positive blood donors* * AABB Chagas Biovigilance reporting system
CDC Nifurtimox releases by year1997 – 2009* Clinical patient releases Blood donor releases * Blood donor screening starts * as of March 25, 2009
Challenges to be addressed • Improve healthcare provider awareness of Chagas disease • Diagnose clinical disease • Recognize transfusion transmission • Screen for transplant transmission risk • Quantify burden of clinical disease in U.S. • Cardiac disease burden • Gastrointestinal disease burden
Risk of Trypanosoma cruzi infection in the U.S. • No estimates because insufficient data • Requires studies to investigate risk of T. cruzi infection by mode of transmission • Autochthonously • During travel • Transfusion-associated • Congenitally
Thanks to • Sonia Kjos, CDC and TX DSHS • Paul Cantey, CDC • Caryn Bern, CDC The findings and conclusions in this presentation are those of the author(s) and do not necessarily represent the views of the Centers for Disease Control and Prevention.