Download
1 / 31
310 likes | 316 Views
Learn about the benefits of oxygen therapy for treating cyanosis and high altitude hypoxia. Understand the symptoms, effects, and acclimatization methods for these conditions.

E N D
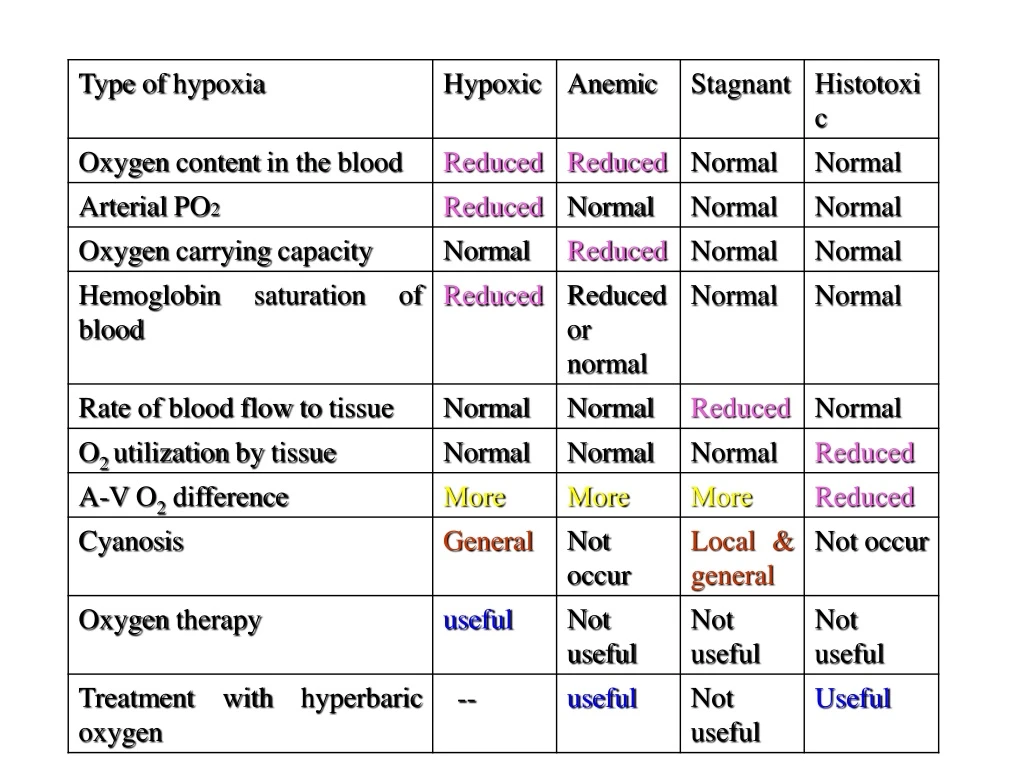
Treatment • Oxygen therapy • Inhalation of 100% pure oxygen. • Inhalation of 100% pure oxygen at high atmospheric pressure-hyperbaric oxygen therapy.
Cyanosis • Bluish coloration of skin, nail beds, ear lobe, lips, fingers & mucus membrane due to presence of deoxyHb >5gm/dl • Local cyanosis or Peripheral cyanosis – seen in stagnant hypoxia due to exposure of cold, circulatory failure • Signs –patients may be cold & blue, peripheral pulses difficult to feel • Central cyanosis – seen in hypoxic hypoxia • Signs –patients extremities are warm & pulsatile, rapid blood flow, increase heart rate & pulse pressure and vasodilation
Before cyanosis readily apparent; the Hb saturation of O2 must fall below 80% & PO2 45 mm Hg. Cyanosis does not occur in – Anemic hypoxia –due to low Hb content CO poisoning –COHb is cheery red Histotoxic hypoxia –O2 utilization is less so HHb is also less High circulatory level of methemoglobin also produce discoloration of skin similar to cyanosis
Role of respiration on acid-base balance: Hypoventilation –retention of CO2 –Respiratory acidosis Hyperventilation –wash out of CO2 – Respiratory alkalosis Metabolic acidosis – pronounced respiratory stimulation —wash out of CO2 –produce compensatory rise in blood pH Metabolic alkalosis –Respiratory depression --accumulation of CO2 –decrease blood pH
High altitude • Atmospheric pressure decreases in high altitude • Concentration of gases everywhere in the atmosphere is same • Whereas, partial pressure of the gas varies. • There is decrease in Partial pressures of oxygen and nitrogen. • As there is not much ill effects due to decrease in partial pressure of nitrogen ,therefore depends on hypoxic conditions (whether onset is sudden or gradual). • Long term stay.(permanent residents).
Hypoxic symptoms at high altitude • Acute mountain sickness -- • Many individuals first arrive at high altitude develops “transient mountain sickness” –acute mountain sickness • The syndrome develops 8 to 24 hours after arrival & last 4 to 8 days
Symptoms of acute mountain sickness are – Less severe hypoxic symptoms – Mental symptoms – Excitement Irritability Mental aberrations such as impaired judgment Disorientation, Loss of sense of time, Loss of sensibility Drowsiness
Severe hypoxic symptoms – 1. Hypertension (proportionate to severity of chemoreceptor drive) 2. High-altitude cerebral edema –due to low PO2 –arteriolar dilation –increase capillary pressure –increase transudation of fluid into brain tissue Due to Cerebral edema – ataxia, disorientation, in extreme case coma & death.
Chronic mountain sickness • Disease of long term residents at high altitude • These people develop –manifestation of superimposed pulmonary disease with -- • Fatigue, reduced exercise tolerance, severe hypoxemia & polycythemia
Acclimatization • Various physiological readjustments and compensatory mechanism in the body to reduce the effect of hypoxia in permanent residents at high altitude. • Increase in pulmonary ventilation. • Decrease affinity of Hb for oxygen under hypoxic conditions.
Polycythemia – due erythropoietin (within 2 to 3 days) –due to hypoxia –sustain as long as stay in high altitude Others – Increase number of capillaries in peripheral tissues Increase mitochondria Increase cytochrome oxidase in the tissue Increase myoglobin level Kidney secrete alkaline urine
Asphyxia • Existence of acute hypercapnia & hypoxia together due to closed airway breathing • Leads to improper aeration of blood • Occur in – • Drowning • Hanging • Pneumothorax
Effect of asphyxia • Stage 1 –Stage of hyperpnoea – • duration 1 min • Features – • Rate & depth of respiration increased • Respiratory efforts are Violent • Dyspnea results • Initially both inspiratory & expiratory movements are increased • Later expiratory movements are more pronounced • Unconsciousness marks end of this stage • Cause –due to hypercapnea
Stage 2 –Stage of central excitation – duration 1 to 2 minutes Expiratory movements are still more pronounced with each expiration, the whole body enters into convulsion Saliva secretion & vomiting occurs Blood pH decreases –acidosis (accumulation of lactic acid due to convulsion) Increased wide spread sympathetic stimulation Signs of central excitations appear – such as Increase heart rate & BP; Pupillary constriction (miosis) Exaggeration of reflexes Cause –hypercapnia, hypoxia & acidosis
Stage 3 –Stage of central depression - Duration 2 to 3 minutes Expiratory convulsion ceases individuals stretches out & open mouth wide as if gasping for breath (gasping type of breathing) Signs of central depression appear – Pupillary dilation . Abolition of reflexes Decreased HR & BP and vasodilation
Periodic breathing • When breathing is non-rhythmic & irregular, it is said to be periodic breathing • Two types • Cheyne-Stoke breathing –Regularly irregular type of periodic breathing • Biot’s breathing –Irregularly irregular type of periodic breathing
Cheyne-Stoke breathingOccurrence of waxing & waning type of respiration with a period of apnea in between last for few seconds to few minutes & then the cycle repeats • Physiological • High altitude • After hyperventilation • In deep sleep • In anesthetic condition • Quite commonin healthy infants • Pathological • Congestive heart failure • Uremia • Elevating intracranial pressure
Biot’s breathing • Varying breathing time alternate with apnoeic periods of different lengths • Transition from periods of activity to apnea & back are abrupt • Occurs only in pathological conditions affect CNS –such as meningitis
Effects of increased barometric pressure (Under water breathing) Increase in atmospheric pressure increases the partial pressure of oxygen and nitrogen. Increase oxygen-oxygen toxicity Increase partial pressure of nitrogen-caissons disease.
Decompression sickness • Caissons disease • Person breathes air under high pressure • Amount of dissolved nitrogen in body fluids increases. • Gets dissolved in fat • Nitrogen narcosis.
Symptoms takes place to a diver, if he ascends rapidly from underwater to surface • In underwater breathing, due to high pressure, volume of gas equilibration (content) in body fluid & tissue is more. • In surface, as pressure is normal, excess gas equilibrates at high pressure begins to come out as bubbles.
Small bubbles –no physiological disturbance Formation of large bubbles (if ascends rapidly) –which when, Coming out in the region of joints –Bends –pain around joints Enter in pulmonary circulation –Chokes –a feeling of shortness of breath often accompanying cough Enter coronary circulation –myocardial damage –heart attack Enter in cerebral circulation –leads to neurological symptoms such as --
Neurological symptoms are – Itching Deafness Impaired vision Vestibular disturbance Even stroke (Diver’s paralysis) In extreme case patient may collapse & die
Prevention – Slow ascends enough to prevent bubbles from being unduly large Wearing SCUBA gear (Self-Contained Underwater Breathing Apparatus) Treatment – Recompression in a pressure chamber followed by slow decompression
Artificial respiration • Useful in– • Acute asphyxia due to drowning • CO or other forms of gas poisoning • Electrocution • Anesthetic accidents
The purpose of giving artificial respiration is -- To maintain the gaseous interchange, the vitality of the nerve centers, as well as that of the heart. It also helps to maintain circulation. It is expected that after sometime, the respiratory centers will start functioning spontaneously. During artificial respiration, the alternate inflation and deflation of lungs reflexly stimulate the respiratory centers, and revived the spontaneous respiration
Methods of artificial respiration • I. Manual methods & • II. Instrumental methods
Manual methods • The different types of manual methods are-- • Schafer’s method- Subject in prone position; Head tilted side; Operator-side by • Holger-Nielsen method (Arm-lift back pressure method) –Subject in prone position, hands folded rested under head; Operator –head end • Sylvester’s method —subject in supine position, Operator at head end • Mouth-to-mouth method –better than others • Eve’s rocking method
Instrumental methods • Negative pressure breathing method – • By alternately compressing and relaxing the chest wall – • Drinker’s method • Bragg-Paul’s method • Positive-pressure breathing – • By introducing air or oxygen directly into the lungs – • Continuous inflation method • Intermittent inflation method
















