Download

1 / 44
480 likes | 673 Views
Unipath 2014. Integrated Diagnostic Services for Haematogical Malignancies - Why wouldn’t you? Robin Ireland King’s Integrated Diagnostic Centre Haematological Malignancy and Bone Marrow Failure Syndromes. What is the problem?. (5 th most common malignancy). Size of the problem.

E N D
Unipath 2014 Integrated Diagnostic Services for Haematogical Malignancies- Why wouldn’t you?Robin Ireland King’s Integrated Diagnostic Centre Haematological Malignancy and Bone Marrow Failure Syndromes
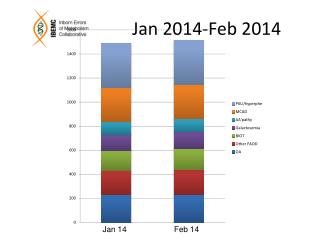
(5th most common malignancy) Size of the problem UK Haematological Malignancy Incidence
Haematological Cancers; estimated annual UK incidence 20,000/yr
12 Major Malignancy Groups (143 subdiagnoses) • Myeloproliferative neoplasms • Myeloid and lymphoid neoplasms with eosinophilia • Myelodysplastic/myeloproliferative neoplasms • Myelodysplastic syndromes • AML • Acute leukaemias of ambiguous lineage • ALL -B and -T • Mature B-neoplasms including all NHL and |Myeloma • Mature -T and -NK neoplasms • Hodgkin lymphoma • Immunodeficiency associated lymphoproliferative disorders. • Histiocytic and dendritic neoplasms.
UK Relative incidences – International geographical variations UK Haematological Malignancy Subtype Data – HMRN
The History of Haematopathology in the UK • The unified concept of haematological malignancy is recent: • Understanding of cellular pathology of the haematopoietic and lymphoreticular systems • UK model dates from the early 1960’s • Pathology subspecialisation • Laboratory Haematology and Histopathology split • Haematologists begin treating leukaemias • Lymphoma and myeloma treated by various specialities • Separation of liquid and solid tissue reporting • Rise of non-morphological techniques • Flow Cytometry • Cytogenetics and Molecular Diagnostics >> FRAGMENTED MODEL
The WHO classification defines diseases as clinico-pathological entities: • Clinical Features • Morphology • Immunohistochemistry • Immunophenotype • Cytogenetics • Molecular genetics
UK NICE Improving Outcomes Guidance: 2003 Diagnosis of Haematological Malignancy • Pathology reviews, audit and trial data suggested significant error rates in diagnosis • Welsh NHS Audit • Accurate diagnosis is increasingly important with changes in treatment and more disease specific directed therapies. • Increasing requirement for cellular prognostic factors and detection of minimal residual disease. • NICE Guidance: ‘Improving Outcomes in Haematological Cancers’ (2003)
USA experience Comparison of referring and tertiary cancer center physician's diagnoses in patients with leukemia. (DeLima M et al. Am J Med. 1998 Mar;104(3):246-51) • 409 patients referred to the M.D. Anderson Leukemia Service • And 100 cases, including 84 of the 409 referred patients for whom the diagnostic outside bone marrow slide had been sent for review. • Overall concordance rate was 73% • 18% discordances were present and considered of major importance (affecting treatment and/or prognosis) • 9% there were minor discordances • Major discordance rates: AML 29% APML 43% MDS 23% CML 5% CLL 2% HCL 57% ALL 19%
Changing Expectation of Diagnostic Services • The Patient and Haemato-oncologist need to have confidence in the accuracy of diagnosis. • The diagnosis needs to be correct and timely. • The morphological opinion of an ‘expert’ is no longer. enough. • Quality is a whole-system process not just NEQAS. • Diagnostic strategies: A systematic approach is essential defining choice and order of testing..
Have raised awareness and improved immunohistological techniques reduced diagnostic errors? 10 years on, is there still a problem? • A recent audit carried out in Greater Manchester (A Norton and R Byers 2008) found the serious and critical error rate to be 15%. These data refer to the diagnosis of lymphoma. • Review was undertaken in a North London Cancer Network. JCO 2011 ……..
Proctor, C. McNamara, M. Rodriguez-Justo, P. Isaacson, and A. Ramsay. Importance of Expert Central Review in the Diagnosis of Lymphoid Malignancies in a Regional Cancer Network, North Central London Lymphoma Whilst error rates have fallen between 2003 and 2008, they are still substantial (13-15%) resulting in minor or major changes in treatment or delay in treatment. Journal of Clinical Oncology April 10, 2011 vol. 29 no. 11 1431-1435
NICE Guidance: Still holds true! • “Improving the consistency and accuracy is probably the single most important aspect of improving outcomes in haematological cancers’’ • “In order to reduced errors, every diagnosis of possible haematological malignancy should be reviewed by specialists” • “Results of tests should be integrated and interpreted by experts” who- -Work with local Clinicians and Pathologists (the final Quality check) to provide a specialised service at network level’
What does this mean in practice? How can it be provided?
Management of patients should be based on sound and comprehensive diagnostic information: An integrated diagnostic process is required Best achieved by co-locating all specialist haematopatholology diagnostic services in a single laboratory. Integration of results into a single final report. Key NICE Recommendations
WHAT IS NEEDED TO MAKE IT WORK? • Agree national model • Identified integrated diagnostic centres • Process of change to implement new model on historical practices and referral practices
An integrated Haematopatholology service is not just an integrated report Multiple levels of integration required. • Integrated approach to the diagnostic process: • Cluster of laboratories and ‘-ologies in an effective diagnostic network • Breakdown historical barriers between laboratories and sub-specialities • Single managerial control, appropriate staffing, organisational and operational structures • Single point of reception for all samples • Design of systematic diagnostic protocols • Integrated IT system • Integrated Final Report combining results from all data sources • Close interface between clinical and laboratory services
Integrated diagnostic processes • Are the best guarantee of diagnostic accuracy based on: • WHO Classification • Systematic diagnostic protocols • Diagnostic protocols designed to give independent checks of diagnosis • Concordance of results across specimen types and diagnostic platforms
A systematic approach is essential • INPUTS: WHO • Clinical Features • Morphology • Immunohistochemistry • Immunophenotype • Cytogenetics • Molecular genetics Accurate Diagnosis Depends on the Integration of Multiple Diagnostic Modalities Immunophenotyping Cytochemistry OUTPUT: The Integrated Report: New diagnoses ICD-O/3 coded Coded comments on: Prognostic factors Minimal Residual Disease monitoring General descriptors Chimerism and Transplant monitoring Free text comments Cytogenetics Morphology Molecular FISH
CURRENT KING’S SERVICES • Fully Integrated Diagnostics and Reporting since October 2007 • Staffing: ~25 staff (Excluding Consultants) • Haematological cytomorphology • Histopathology/Immunohistochemistry/Cytopathology • Flow Cytometry • Cytogenetics/FISH • Molecular Diagnostics • IT and other infrastructures.
Adult Population ~5.3m ~12,000 referrals and ~22,000 tests King’s Haematological Malignancy Diagnostic Centre • All haematological malignancies: Acute, Chronic, Myeloid, Lymphoid, Plasma Cell, Histiocytic, Dendritic. • 3 Cancer networks • 17 Hospitals • Specimens: • Peripheral blood • Marrow Aspirate and Trephines • Tissue biopsies; Ln’s, extranodal, skin, lung etc • CSF/Vitreous Humour /Ascites/Pleural/ Pericardial fluids.
WHAT IS NEEDED TO MAKE IT WORK? • Laboratory services and staff need to be robust and flexible: • Rapid development/implementation of new technologies • Challenges traditional technical/-ology borders • Platform of technology research feeding diagnostic service • Changes in skill mix and cross-cover. • Capital investment capability
Integrated Haematopathology Services: - Organisation • A single Centre with overall responsibility: • Operational, managerial and financial • Identified laboratories and investigational modalities. • Minimum catchment population • May provide services to more than one Network • Management and organisational accountability • Single Head of Service • Defined role and responsibilities including: • Design of algorithms • Resource utilisation • Links with clinicians • Specimen(s) sent to a single reception point • Identified optimal samples, methods of handling and transport • Speedy transfer of samples to minimise delays of diagnosis • Prevent omission of key tests and over-investigation
IMPROVED PROCESSES Referred Samples IHMDC Reception NHS No. or Lifelong and Event Specific ID Finite cell samples – use to maximum diagnostic benefit in shortest possible time. Most samples come with diagnosis of ‘cytopenia or splenomegaly ? Cause. Even if given a diagnosis, often incorrect!! Cytogenetics /FISH Result Molecular Genetics Result Histopathology /Cytology Result Morphology/ Immunopheno -typing Result Initial review determines downstream investigations Consultant Worklist Trafficlight results status Integrated Results ICD-O/3 Codes Interpretive comments Interim/Final Report Authorised Paper and Electronic issue
KCH Sample flows 2013 – Centralised model Single Reception > Testing > Integrated Report
WHAT IS NEEDED TO MAKE IT WORK? -Information Technology Systems • I.T. software is the ‘glue’ that makes it a workable and effective system: • Patient, clinical and sample details recorded. • Investigative protocols: • Systematic, sequential test ordering protocols • Worksheet generation • A single integrated report linking all results. • Communications with users: • Single point direct access • Use of e-mail alerts and electronic return of results. • Quality assurance and audit
Referred Samples HMDC Reception NHS No. or Lifelong and Event Specific ID Cytogenetics /FISH Result Molecular Genetics Result Histopathology /Cytology Result Morphology/ Immunopheno -typing Result Initial review determines downstream investigations Consultant Worklist Trafficlight results status Final check of result quality, internal consistency, concordance or DISCORDANCE of results Integrated Results ICD-O/3 Codes Interpretive comments Interim/Final Report Authorised Paper and Electronic issue
WHAT IS NEEDED TO MAKE IT WORK? - Quality Assurance • Quality and governance built into the system, facilities and processes. • Standard Operating Protocols for order and choice of tests. • Accuracy of reporting: • Double reporting/authorisation • Result concordance • CPA, NEQAS, EQA • Monitoring of reporting times • Monitoring of resource utilisation and efficiency.
Supporting structures • Education and training: • Technical/Scientific • Postgraduate: Trainee Registrars all rotate into HMDC • Consultants
Key Requirements: R&D Infrastructure • Diagnostic Techniques are changing rapidly: • Relative decline of morphology (remains an important triage step) • Multicolour flow techniques (8 – 10 colour). • Gene expression profiling, Deep Sequencing capabilities, SNP-A karyotyping, miRNA’s, whole exome sequencing etc. • Diagnostic services underpinned by large R&D infrastructure and capability. • New skills required – Bioinformatics and mathematical algorithms • Clinical needs are evolving: • New treatments and monitoring should be seen as a package • Eg CML and BCR-ABL/ABL ratios • Centre for Clinical Trials in Haematological Malignancies. • Now incorporated into Current trials – e.g. REMoDL-B…….
Concerns – Role of District Hospital Haematologists • Haematologists should still report their own aspirate/trephine slides. • Local Haematologists do not usually undertake the specialist tests (Immunophenotyping, Cytogenetics, FISH, Molecular Genetics) so for the majority this is not a real change. • If there are haematologists/histopathologists who have a mainly Haem-Oncology laboratory role they could/should be incorporated into the provision of services centrally: • Cancer Pathology Commissioners and Hospitals must be brought into the discussions so that relevant consultants can participate in diagnostic service provision. • Will see more and access a wider range of diagnostic technologies.
Concerns - Deskilling • Clinicians can and should still combine their clinical and laboratory skills. • They should continue to report bone marrows; this is an important quality assurance step where treatment decisions are made. • IOG clarification is not about morphology skills of haematologists (which they are encouraged to maintain) but is about the proper integrated diagnostic process of specialist testing - core to the NICE guidance.
The case for a centralised model Why would you leave a distributed (fragmented) service model? • Difficult to implement modern, complex, integrated diagnostic approaches. • Complex transport arrangements, delays, risks of sample loss. • Many cases come without a firm or correct diagnosis: • Slow/difficult communication between labs to change investigations. • Slow to switch samples between labs; sample degradation and lengthened delays. • Inability to discuss results from discordant cases with all slides/ results/people simultaneously. • Inhibits cohesion, communication, coordination and teamwork • Inefficient utilisation of scarce staff resources and skills • Compromises critical mass for development, learning and research • No multi-tasking and multi-skilling = Inefficient labour force • Does not facilitate service delivery, teaching, tissue banking or research.
Patient/Clinician/Organisation Who wants? • A slow result with a 10 – 25% error rate? • Laboratory reduplication with high capital costs? • Inefficient use of resources/high revenue costs? • Non-robust staffing? • No multiskilling? • Slow implementation of technologies? • Poor training? • Defunct research? - - especially molecular capability.
THANK YOU HAEMATOLOGISTS Prof G Mufti Dr R Ireland Dr V Tindell Dr D Yallop Dr S Kassam HISTOPATH J Salisbury S Pomplun C Shah H Abu-Arqoub J Morehead CYTOGENETICS B Czepulkowski L Brown P Ford H Gilbert T Kontou D Ladon V Simonian D Jijon FLOW CYTOMETRY Tim Milne Anne Etches Melissa Bullard Debbie D’Costa MOLECULAR Nic Lea A Kizilors N Folarin S Best J Anwar RECEPTION C Sulzdorf R Connell