Download
1 / 42
420 likes | 577 Views
CNS DEGENERATION. FM Brett MD., FRCPath. At the end of this lecture you should be able to: Understand the definition of dementia Be able to list the common causes of dementia Understand Parkinson’s Disease Understand what is meant by Multiple Sclerosis. DEMENTIA.

E N D
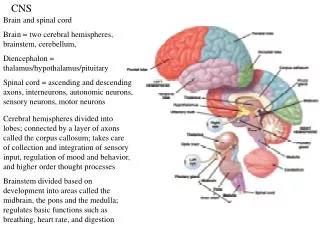
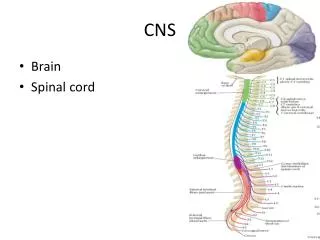
CNS DEGENERATION FM Brett MD., FRCPath
At the end of this lecture you should be able to: • Understand the definition of dementia • Be able to list the common causes of dementia • Understand Parkinson’s Disease • Understand what is meant by Multiple Sclerosis.
DEMENTIA • Acquired global impairment of intellect memory and personality • Impairment of intellectual function in the presence of normal consciousness affecting • Language • Visuospatial skills • Emotion or personality • Cognition
Dementia Distinguished from mental retardation on the basis of having attained an appropriate degree of occupational and social functioning Presence of multiple cortical defects implies involvement of multiple cortical areas
Prevalence • at least 2% at age 65-70 • 20 % at age 80
Exclude Temporary confusion Primary memory loss
Common causes of dementia Neurodegenerative – common – AD DLBD CVS - multi-infarct dementia Hydrocephalus Toxic and metabolic Drugs Alcohol Mitochondrial encephalopathy Demyelinating disease Head injury Prion diseases Infective – HIV, neurosyphylis Neoplasia – paraneoplastic syndromes
Alzheimer’s Disease ~ Commonest cause of dementia ~ 50-75% of all cases of dementia ~ 5 groups ~ Sporadic late onset (commonest) ~ Familial late onset (uncommon) ~ Familial early onset (rare) ~ Associated with Down’s syndrome ~ Associated other degenerative disease
Molecular pathology of AD AD1 mutations in the APP on Ch21 AD2 ass with the APOE4 allele on Ch 19 AD3 associated with the presenilin 1 gene on Ch 14 AD4 mutation in the presenilin 2 gene on Ch 1
CAUSES OF PARKINSONISMCOMMON – PD LESS COMMON – Drug induced, MSA, PSP, vascular RARE - CBD, AD, MSD, hydrocephalus, FTD, HC, Dementia pugilistica, toxins,
Parkinson’s Disease Clinical diagnosis REQUIRE 2 of the 3 cardinal features Bradykinesia Resting tremor Rigidity Associated features: Autonomic dysfunction Cognitive disturbance Dysphagia
Manifestations of PD largely attributable to reduced dopaminergic input into the striatum due to degeneration of neurones in the pars compacta of the SN Genetic Free radical damage Environmental agents
DLBD Progressive cognitive decline • + two of the following • Fluctating cognition • Recurrent visual hallucinations • Spontaneous motor features of Parkinsonism
DLBD Supportive features – Repeated falls Syncope Neuroleptic sensitivity Systematised delusions Hallucinations
Frontotemporal dementia Patients presenting with progressive frontal lobe dysfunction (that may later be followed by evidence of temporal lobe dysfunction) Accounts for 10% of all cases of dementia
Vascular Dementia ~ Cumulative cognitive decline caused by effects of multiple episodes of cerebral ischaemia ~ Excludes cases caused by diffuse cerebral cortical damage due to a single episode of severe hypoxia or global cerebral hypoperfusion
Classification of demyelinating disorders of the CNS • Primary demyelinating diseases – MS, ADEM, AHL • Secondary demyelinating diseases CPM, PML, SADC, • Leukodystrophies and metabolic disorders e.g sudanophilic leucodystrophy, metachromatic leucodystrophy, adrenoleucodystrophy, Krabbes leucodystrophy, Canavans disease • Toxic demyelination - Hexachlorophane, cyanide, carbon monoxide, chronic solvent vapour abuse.
MS • Chronic, progressive immune-mediated CNS disease • Characterized by demyelination and axonal loss neurologic impairment and disability • Axonal damage and brain atrophy occur earlyand may be irreversible
~ 85 % RRMS i.e sporadic attacks followed by complete, partial or no improvement ~ Within 10 years half of these pts develop secondary-progressive disease (essentially unrelenting clinical progression with possible superimposed acute attacks and minor remissions) ~ Remainder primary-relapsing disease – characterised either by progression from onset with acute relapses OR Primary progressive disease progression without relapse or remission
Epediomology of MS • ~350,000 affected in US • ~8,500–10,000 new cases yearly • Most cases strike between ages 15 and 45 • Women outnumber men 2:1 • 85% present with RRMS • Within 10 years, 50% of these patients develop secondary-progressive MS associated with significant disability
Presenting features of MS Limb weakness 50% Optic neuritis 20% Diplopia 10% Parasthesia 10% Bladder Parasthesia 10% Vertigo and nystagmus 5%
Diagnosis of MS Dissemination of lesions in space Dissemination of lesions in time Paraclinical tests VER, MRI Clinical history Less commonly acute mass lesion difficult to distinguish clinically and pathologically from a neoplasm
MS Characteristics 2. Characterized by demyelination and axonal loss neurologic impairment and disability 1. Immune-mediated CNS disease 3. Dissemination of lesions in space
Normal white matter Active demyelination Inactive plaque
Normal white matter Active demyelination Inactive plaque
Biopsy F23 Ambulant 14 yrs later F21 wheelchair bound F 36 Died 56 dys after admission
Normal white matter Active demyelination Inactive plaque
Pathological features of acute demyelination Hypercellularity – macrophages +++++ Areas of complete myelin loss Relative axonal preservation Perivascular lymphocytic cuffing Annesley-Williams et al., JNEN 2000;59:477-89
Diagnosis of MS Dissemination of lesions in space Dissemination of lesions in time Paraclinical tests VER, MRI Clinical history Less commonly acute mass lesion difficult to distinguish clinically and pathologically from a neoplasm
Central Pontine Myelinolysis ~ Middle aged or elderly patients who are malnourished or chronically debilitated ~ Associated with fluid-electrolyte imbalance particularly where hyponatremia has been treated rapidly with hypo-osmolar saline ~ Mechanism of demyelination is unknown but may relate to impaired vascular perfusion during the episode of rapid electrolyte shift ~ Myelin loss usually occurs in the central pons
Progressive Multifocal leucoencephalopathy ~ Lytic infection of oligodendrocytes by JC virus ~ Usually debilitated or immunosupressed patients ~ well recognised complication of Aids
CONCLUSION: • Dementia is… • Commonest cause worldwide is Alzheimer’s Disease • Commonest cause of PD is idiopathic • Incidence of CJD is 1 per million worldwide per year. • Diagnosis of MS is based on dissemination of lesions in time • (clinical history) and space (based on appropriate paraclinical • tests)