Download
1 / 34
340 likes | 342 Views
Implications of the Supreme Court ACA Ruling on Medicaid Expansion. Paul Gionfriddo Our Health Policy Matters http://pgionfriddo.blogspot.com Mental Health America Webinar Briefing August 9, 2012. The SCOTUS ACA Decision.

E N D
Implications of the Supreme Court ACA Ruling on Medicaid Expansion Paul Gionfriddo Our Health Policy Matters http://pgionfriddo.blogspot.com Mental Health America Webinar Briefing August 9, 2012
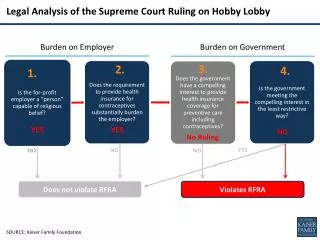
The SCOTUS ACA Decision • Individual mandate is constitutional because it is a tax, not as a “command” under Commerce Clause. • Mandatory Medicaid expansion is unconstitutional; states can opt out of expansion and keep their existing Medicaid programs. • Unconstitutional portion is severable from the rest of the law.
What the Court Found Re: Medicaid Expansion “Nothing in our opinion precludes Congress from offering funds under the Affordable Care Act to expand the availability of health care, and requiring that States accepting such funds comply with the conditions on their use. What Congress is not free to do is to penalize States that choose not to participate in that new program by taking away their existing Medicaid funding.” Roberts Opinion, p. 55
ACA Projected 2022 Effect on Insurance Coverage, Before Ruling(CBO, 2012, numbers in millions)
ACA Projected 2022 Effect on Insurance Coverage, After Ruling(CBO, 2012, numbers in millions) 6 3 3
CBO: Court Ruling Created Three Probable State Options • Full Expansion – expansion to 138% of poverty. • No expansion – leaves current program in place. • Partial Expansion – expansion for some groups, or to less than 133% of poverty? Sara Rosenbaum, JD, GWU: “…nor is there anything in the description of the 2014 mandatory expansion group as it stands both before and after NFIB v Sebelius that would suggest that such flexibility suddenly has appeared.” (Health Affairs, 7/31/12)
States Currently Considering Rejection of the Medicaid Expansion Governors: Reject It • #19 Iowa • #33 Florida • #40 South Carolina • #42 Texas • #44 Louisiana • #47 Mississippi Governors: Wait and See • New Jersey • Utah • Wisconsin • Virginia Note: Numbers represent preliminary Our Health Policy Matters State Health Rankings for 2012
Medicaid Expansion Rejection Effect on 3 Groups • People will be harmed. • Providers will be harmed. • States and their budgets won’t be helped.
People Effect: Who Gets Hurt? • “Most of the new enrollment projected to occur under the ACA’s Medicaid expansion is expected to be among childless adults and parents who are not already covered under their state’s eligibility rules.” Source: CBO Estimates for the Insurance Coverage Provisions of the Affordable Care Act Updated for the Recent Supreme Court Decision, July 2012
People Effect: If Medicaid Expansion is Rejected… • Exchange subsidies begin at 100% of poverty. People below 100% of poverty will not be eligible for any exchange subsidies. • Between 100% and 133% of poverty, people will have to pay 2% of income toward premiums. • Medicaid expansion included 5% income disregard (making people up to 138% of poverty eligible), but ACA exchanges do not include this disregard.
Provider Effects: Why Medicaid Matters to Safety Net Providers
Provider Impact of Expansion Rejection • ACA cuts $10 billion in Medicare and Medicaid Disproportionate Share Hospital (DSH) payments as of 2018. Hospitals will still lose DSH payments in states that don’t expand Medicaid. • Community health and mental health centers will lose a revenue stream for comprehensive and integrated care to adults with chronic conditions. • Behavioral health programs lose $$$ to replace $3.4 billion cut by states between 2009 and 2012.
State Budget Effects: Projected Growth of Medicare and Medicaid Federal 61%
Governors Claim High Cost of Medicaid Expansion • “Florida estimates that, as a result of the ACA, its share of Medicaid spending will increase by $1 billion annually by the end of the decade.” • “Louisiana anticipates additional spending of approximately $7 billion over ten years.” • “Texas anticipates additional annual spending of $1 billion in 2014–16, $2.1 billion in 2017–19, and $4.4 billion annually thereafter.” Source: Supreme Court Brief of State Petitioners on Medicaid, January 10, 2012, p. 17
Governors Inflate ACA Medicaid Cost by Including Currently Eligible Source: FL Attorney General Pam Bondi, Supreme Court Brief, 2012
Federal Share of Medicaid Expansion It is a misconception that the federal 90% match is not permanent. It is in fact as permanent as the program itself.
More Uncertain Effects of Expansion Rejection • Because Roberts defined the expansion as a “new program:” • New Medicaid “Basic Benefits” package is at risk. • New Medicaid mental health parity and prescription drug coverage provisions are at risk.
Key Advocacy Message Frames • This is a marathon, not a sprint. No matter what the governors say, nothing is a done deal until 2014 or beyond. • Tell your own stories. Make the impact real. • Focus on unintended consequences of failure to expand, such as effects on hospitals and poor seniors. Don’t fear scary. • Use media you control – Facebook, Twitter, Email, LinkedIn – to counter bad information and build support for the expansion, and use these frequently. Once is not enough. • Half a loaf is better than none. Partial expansion is better than no expansion at all.
“His Own Heart Laughed: and That Was Quite Enough For Him.” Thank you! http://pgionfriddo.blogspot.com gionfriddopaul@gmail.com
Advocacy Strategies Making the case in your state for Medicaid expansion. National Health Law Program: 10 Advocacy Steps To Support A Medicaid Expansion in Your State http://www.healthlaw.org/images/stories/10_Advocacy_Steps_for_Medicaid _Expansion_07_06_2012-1.pdf
Medicaid expansion is free for 3 years • For current Medicaid – an average of 57% of Medicaid costs is paid by the Feds • For expansion – 100% Federal dollars in 2014, 2015, and 2016 Messaging • In difficult financial times, our state cannot afford to leave free money on the table. • Our state has free money available to cover uninsured people. The Governor is engaging in political posturing when she says she is going to turn the money down. • We pay federal taxes – why should citizens of our state continue to go without insurance while other states reap the benefits of our taxes?
After 2016, it’s still a great deal • Some argue that it’s a great deal for the first 3 years but states can’t afford it after that. Reality…. • For current Medicaid – an average of 43% of Medicaid costs are paid by the states • For the expansion – states pay 5% in 2017, 6% in 2018, 7% in 2019, and then 10% in 2020 and beyond. • The most states will ever pay is 10% of cost Messaging • Every state voluntarily pays on average 43% of the Medicaid bill, so paying 10% for the expansion population is reasonable. • Medicaid is a joint state-federal program, and in this case the federal government is willing to pay 90% of the costs. This is a really favorable partnership for the state.
Provide context for budgetary numbers • Policy makers may throw out large number for the cost of the expansion – e.g. $10 billion over the next decade • It may help to put those numbers in perspective – as the percentage of the Medicaid and/or state budget and accompany those numbers with the percentage of people who will gain coverage • KFF document shows state-by-state the percentage of people gaining coverage, costs to state, costs to feds - http://www.kff.org/healthreform/upload/Medicaid-Coverage-and-Spending-in-Health-Reform-National-and-State-By-State-Results-for-Adults-at-or-Below-133-FPL.pdf Messaging • The cost of this program represents __% of our current Medicaid (or state) budget and for that money we would cover __% more uninsured people.
Correct bogus numbers • Some policy makers are exaggerating expansion costs by including already eligible enrollees into their costs • Enrollment in traditional Medicaid is expected to grow – but it is a different program • Remind policy makers of the lost revenue due to the reduction in DSH payments Messaging • The Governor quotes a cost of $3 billion dollars, but that includes $1 billion dollars for people already eligible and the state had simply failed to enroll. • Even if the state doesn’t opt for the Medicaid Expansion, the state Exchanges will be starting at the same time. When these people who are already eligible go to the Exchange, they will be referred to the Medicaid program and come into the system anyway.
Medicaid Expansion saves state money • States will realize savings in programs that are currently used by the uninsured. • Many of these programs are solely or jointly funded by county and/or municipal governments. • Identify state and local programs that will save money from the expansion and how the costs will be offset. Messaging • Covering the uninsured population in our state will save the state millions of dollars spent on uninsured people in the state-funded health care programs and will save millions of local dollars spent in the county mental health system. • Local CHCs will be able to bill Medicaid for the uninsured patients they currently see using state and local dollars. • Everyone in the state will save money, because hospitals will stop passing on to everyone else the costs of providing care to uninsured individuals.
State savings continued • It can be argued that state savings can also be realized in non-health expenses when mental health and substance use are covered • Access to mental health treatment can impact other state budget lines that don’t have a federal match; homelessness services, criminal justice*, tax revenue Messaging • The state is spending millions/billions on non-health related services, especially in the corrections system, that could be mitigated if people had coverage for mental health and substance use services. • When people leave jails or prisons, they don’t have access to insurance and therefore can’t continue the treatment that has helped them get better. Expanding Medicaid would provide continuity of care and keep people from cycling back into the costly corrections system. *West, J.C., et al. (May 2009). Medication Prescription Drug Policies and Medication Access and Continuity: Findings From Ten States. Psychiatric Services. Vol. 60, No. 5.
Effects on the state economy • An insured workforce gets more medical attention, is healthier and more productive • Employers with lower wage and part time workers will benefit from covered workers • More people access medical coverage means business for providers, clinics, health systems, insurers, helping the state and local economy Messaging • As sick workforce is less productive. The Medicaid Expansion will improve the health of workers in our state, and this has been shown to boost productivity. • The health industry is an important part of state and local economies, and the Medicaid Expansion will increase business in the health industry and stimulate the state economy.
Medicaid is the best coverage • Medicaid benefits have been designed to meet the needs of low-income individuals and is therefore the best coverage for this population. • Expansion benefits include the benefits in the Exchange and have flexibility to add more. • Those who sign up for new Medicaid but are categorically eligible will get the more robust benefits. • The individuals below the poverty line often live in very poor health and are more likely to have mental health conditions, and Medicaid benefits are specifically designed to meet the needs of low-income people with serious health care needs.
Medicaid is the mostaffordablecoverage • Medicaid has protections to limit premiums, deductibles, copays, and cost-sharing • The Exchange will not have those same limitations Messaging • The Medicaid Expansion is the best way to cover low-income individuals because Medicaid is designed to be affordable for low-income families, meaning people can afford to go to the doctor when they get sick.
Medicaid is the mostaffordable option for the government • Medicaid is the least expensive health insurance program in the country. • Medicaid is by far the least expensive way to cover low-income individuals and is far less expensive than providing coverage in the Exchange. • Relying on the Exchange to cover low-income individuals rather than Medicaid puts 100% of the costs of a higher cost option on the federal government. Messaging • Medicaid is the least expensive way for the government to provide coverage for low-income individuals. In fact, it is three times more expensive for the government to cover individuals through the Exchange.
Coalitions of stakeholders • Those with common interests: hospital associations (lost DSH payments), community health centers, public health workers • Managed care organizations, business community (maybe?) Messaging • There is broad support across the state, including individuals, doctors/providers, hospitals and health systems, and businesses, for the state to implement the Medicaid Expansion.
Medicaid saveslives July New England Journal of Medicine article • Study of mortality rates for people age 20-64 in 3 states (NY, ME, AZ) with Medicaid expansions decreased by approximately 1,500 deaths per year. • Adjusted for income, unemployment, age, sex, and race – decline of 6.1% in deaths Prelim data from Oregon study • Expanded Medicaid for 10,000 people in 2008 • Data showing Medicaid population see doctors more often, report better health, and better financial stability Messaging • The Medicaid Expansion will reduce premature mortality for non-elderly adults in our state, and will allow our citizens to see doctors when they need to, have better health, and experience financial stability.
OtherStrategies & Messages Questions, Comments, Thoughts? Sarah Steverman 703.797.2594 ssteverman@mentalhealthamerica.net