Download
1 / 62
1.06k likes | 2.05k Views
Maintenance of anesthesia. Kelly Shinkaruk, MD FRCPC HLT 123 October 17, 2009. Objectives. What is anesthesia? Manual monitoring techniques Inspection Palpation Auscultation Evaluation and maintenance of anesthetic depth using Non-invasive monitors Invasive monitors

E N D
Maintenance of anesthesia Kelly Shinkaruk, MD FRCPC HLT 123 October 17, 2009
Objectives • What is anesthesia? • Manual monitoring techniques • Inspection • Palpation • Auscultation • Evaluation and maintenance of anesthetic depth using • Non-invasive monitors • Invasive monitors • Nervous system monitors • Adjusting medications to maintain anesthetic
Objectives • What is anesthesia? • Manual monitoring techniques • Inspection • Palpation • Auscultation • Evaluation and maintenance of anesthetic depth using • Non-invasive monitors • Invasive monitors • Nervous system monitors • Adjusting medications to maintain anesthetic
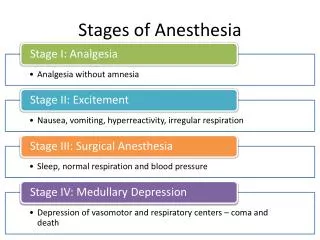
What is anesthesia? • “…drug induced reversible depression of the central nervous system resulting in the loss of response to and perception of all external stimuli.” • Components of anesthesia • Unconsciousness • Amnesia • Analgesia • Immobility • Attenuation of autonomic response to noxious stimulation
Goals of Maintenance • Responsible for autonomic nervous system • Maintenance throughout case of • anesthesia • amnesia • analgesia • paralysis (if indicated) • In addition • Minimize negative effects of anesthetic • Fluid maintenance/balance/resuscitation • Cardiac output and end organ perfusion
Goals of Maintenance • Why use monitors? • Detect deficit or overdose of anesthetic agents and resolve the aberrancy • Early detection of adverse events • Prevention of periop critical events • Prior to advent of standard monitoring, anesthesia had very high morbidity and mortality • Now it’s very low
CAS Monitors • Use monitors to help narrow your differential diagnosis • No single monitor can make a diagnosis, must verify one monitor with another!
Depth of Anesthesia • If monitored vitals change • Consider differential diagnosis • Simultaneously manage and diagnose • ABCs, verify result with another monitor • Inspect, palpate, auscultate • Make adjustments to medications as appropriate!!!
Objectives • What is anesthesia? • Manual monitoring techniques • Inspection • Palpation • Auscultation • Evaluation and maintenance of anesthetic depth using • Non-invasive monitors • Invasive monitors • Nervous system monitors • Adjusting medications to maintain anesthetic
Manual Monitoring Techniques • “The only indispensable monitor is the presence, at all times, of a physician or an anesthesia assistant, under the immediate supervision of an anesthesiologist, with appropriate training and experience.” • CAS guidelines 2008 • Provides valuable information about • Depth of anesthesia • Diagnosis of intraoperative complications
Manual Monitoring Techniques • Inspection (Adequate Lighting) • Historically, sole monitor • Initial information by observation • Inspect for alterations • Diaphoresis • Spontaneous movement • Respiratory rate and pattern esp. when spontaneous • Abnormal retractions or indrawing • Cyanosis • JVP • Skin colour and/or rash
Manual Monitoring Techniques • Palpation • Correlate information from inspection • Physical contact with patient • Palpate for • Tracheal position • Subcutaneous emphysema • Pulsus paradoxus • Heart rate, rhythm, contour
Manual Monitoring Techniques • Ausculation (Stethoscope!!!) • Respiratory system • Endotracheal tube placement/malposition • Wheezes/crackles • stridor/decreased air entry • Cardiovascular system • Murmurs/bruits • Changes in quality of heart sounds (S1, S2, decreased heart sounds)
Objectives • What is anesthesia? • Manual monitoring techniques • Inspection • Palpation • Auscultation • Evaluation and maintenance of anesthetic depth using • Non-invasive monitors • Invasive monitors • Nervous system monitors • Adjusting medications to maintain anesthetic
Non Invasive Monitors • Pulse Oximetry • Simple, noninvasive, continuous • indirectly measures the oxygen saturation of a patient's blood • Detect and prevent hypoxemia • Affected by • dyshemoglobins, vital dyes, nail polish, ambient light, motion artifact, background noise/electrocautery
Non Invasive Monitors • Pulse Oximetry • When sats fall, differential diagnosis • Low FiO2 (relative or absolute) • Inadequate alveolar ventilation • V/Q mismatch • Excessive metabolic O2 demand • Low cardiac output • Treatment? • 100% O2 • Increase ventilation rate/Vt or change vent mode • Recruitment maneuvers
Non Invasive Monitors • Blood Pressure (via cuff) • Indicates adequacy of circulation • Minimum monitoring interval - 5min • Monitor location – upper arm, leg, forearm
Non Invasive Monitors • Blood pressure • Hypertension diagnosis? • Light anesthesia • Catecholamine release • Laryngoscopy • Surgical stimulation • Emergence from anesthesia • Administration of vasopressors • Treatment? • Deepen anesthetic • d/c vasopressors
Non Invasive Monitors • Blood Pressure • Hypotension differential diagnosis? • Is extensive… • Hypovolemia • Relative overdose of anesthetic agents • Treatment? • Initially, go through ABCs, inspect for evidence of bleeding, 100%O2, turn down anesthetic • Fluid bolus – NS/RL 500-1000mL • Vasopressor – Phenylephrine 100mcg or Ephedrine 2-10mg
Non Invasive Monitors • Electrocardiogram • Three or five leads • Continuous measurement of heart rate and rhythm • Questionable indicator of myocardial ischemia • Signs of light anesthesia • tachycardia • Might notice changes in rhythm • Vasovagal episodes • Tell surgeon to STOP!!! • Atropine 0.4mg or Ephedrine 5-10mg
Non Invasive Monitors • Expired Agents/Gases • The most important objective indicator of depth of anesthesia • Monitors the concentration of gas (volatile, CO2, O2) being expired from the patient • MAC (minimum alveolar concentration) = 50% of people will not move with surgical stimulus • Monitor end tidal concentration of agents
Non Invasive Monitors • Expired Agents/Gases • MAC is affected by many things • Intravenous medications – PPF, opioids, benzos • Pre-op medications – pregabalin, benzos • Age • Medical conditions/patient health • Hypo/hyperthermia
Non Invasive Monitors • Expired Agents/Gases • If low and patient appears light • Increase flow rate • Increase percent of volatile delivered from vaporizer • Make sure to monitor MAC as can increase rapidly! (and cause hypotension)
Non Invasive Monitors • Capnography • Insp/exp CO2 concentration • Vital monitor of physiology • Confirm ETT placement • Recognize ETT malposition/extubation/disconnection • Assess adequacy of ventilation/PaO2 • Aids diagnosis of PE, partial A/W obstruction, RAD/bronchospasm • Assess efficacy of CPR efforts
Non Invasive Monitors • Capnography • If increased ETCO2 • Check CO2 absorber! • Increase minute ventilation (RR or Vt) • ?hypermetabolic process? • If decreased ETCO2 • Sudden vs slow • Decrease ventilation • Verify other signs of hypoperfusion
Non Invasive Monitors • Respiratory Function • Especially useful in spontaneously ventilating patient • Light patient • Hyperventilation - increased RR/Vt and hypocapnia • Breath holding • Bronchospasm/laryngospasm • Very deep patient • Hypoventilation – decreased RR/Vt and hypercapnia
Non Invasive Monitors • Increase in respiratory rate • Differential mainly light anesthetic and hypoventilation • Increase ventilation (RR or Vt) • Deepen anesthetic • Administer analgesic
Non Invasive Monitors • Ventilator Pressures • Early indication of light anesthetic and other problems! Always check: • Breathing circuit • ETT • Pulmonary compliance • Alarms for increased pressure • Coughing • Insufficient muscle paralysis • Bronchospasm • Obstruction/pt biting ETT
Non Invasive Monitors • Ventilatory Pressure elevated • Differential diagnosis • Manage and diagnose • Inspect patient and ETT – biting, blocked, disconnected (if low pressure alarm) • Take off machine and verify compliance • Auscultate breath sounds – ETT malposition • Treatment • Deepen anesthetic • Paralysis • Reposition/Suction/change ETT
Non Invasive Monitors • Temperature Monitoring • Can be monitored via bladder, distal esophagus, ear canal, trachea, nasopharynx, rectum • Attempts made to maintain temperature as close to normothermia as possible • Situations requiring temp monitoring • Long cases • Anticipated fluctuations in temperature • Bair hugger • Malignant hyperthermia patients
Invasive Monitors • Arterial Line • Continuous blood pressure measurement • Placed in a peripheral artery • Radial • Brachial • Dorsalis pedis • Rarely femoral • Waveform gives information about intravascular status • Help with diagnosis of cardiac tamponade,etc
Invasive Monitors • Arterial line • Indications: induced hypotension, induced hypothermia, major cardiac/thoracic/vascular/neurosurgical procedures • Always keep BP cuff in place for verification of arterial BP • Used for frequent blood sampling esp. ABGs • Be aware that tracing can be damped/positional • Flattened waves might be artifactual • Verify with BP cuff
Invasive Monitors • Central Venous Pressure (CVP) • Estimates of right atrial/ventricular pressures • Serial measurements more useful than single value • monitor intravascular volume/fluid status • Renal failure patients • Difficult IV access • Anticipated need for vasopressor infusion/TPN/Hemodialysis • Massive transfusion
Invasive Monitors • Pulmonary Artery Catheter (PAC) • Rarely indicated, TEE rapidly replacing • Inflation in pulmonary artery reflects left atrial filling pressure • Can calculate cardiac output • High risk of complications • PA rupture • PVCs/Vtach • Hemo/pneumothorax
Invasive Monitors • Transesophageal Echo • Echo probe placed in esophagus during GA • Uses ultrasound technology • Assess cardiac function/filling/valves • Replacing PAC technology • Requires special equipment
Invasive Monitors • Evaluation of • Native valve disease • Prosthetic heart valve function/dysfunction • Cardiac masses • The ICU patient with hemodynamic instability • Congenital heart disease • Thromboembolic risk in patient with atrial fibrillation and inadequate anticoagulation • Detection of • Aortic dissection • Complications of endocarditis • Potential etiologies of stroke • Adjunct to • Percutaneous cardiac procedures • Cardiac surgical procedures
Invasive Monitors • Heart valve repair • Most congenital heart surgery requiring cardiopulmonary bypass • Endocarditis, particularly with extensive disease or inadequate preoperative evaluation of disease extent • Ascending aortic dissection repair when aortic valve involvement unknown • Evaluation of life-threatening hemodynamic disturbances when ventricular function is unknown • Pericardial window procedures • Hypertrophic obstructive cardiomyopathy repair • Heart valve replacement • Removal of cardiac tumors • Increased risk of myocardial ischemia or hemodynamic disturbances • Intracardiacthrombectomy or pulmonary embolectomy • Suspected cardiac trauma or for detection of foreign bodies • Cardiac aneurysm repair • Thoracic aortic dissection repair without suspected aortic valve involvement • Evaluation of anastomotic sites during heart and/or lung transplantation • Monitoring placement and function of assist devices
Nervous System Monitors • Electroencephalogram (EEG) • Represents spontaneous electrical activity of the cerebral cortex • Measures amplitude and frequency of discharge • Four frequencies: beta, alpha, theta, delta
Nervous System Monitors • Electroencephalogram (EEG) • EEG may be used to detect intraop cerebral ischemia • Deep anesthesia and cerebral ischemia decrease or abolish normal alpha/beta; delta/theta predominate
Nervous System Monitors • Bispectral Index (BIS) • A variable derived from the EEG • Measure of the hypnotic effect of anesthetic • Gives a value between 0 and 100 • Decreasing numbers = deeper anesthetic • <60 appears to predict unconsciousness • Used in trauma, crash OB, cardiac, unstable patient with minimal reserve/anesthetic