Download
1 / 15
150 likes | 234 Views
The Broadband and E-Health December 2009. The Australian e-Health Research Centre. Joint Venture between CSIRO and the Queensland Government (2003) Leading national research facility in ICT for healthcare innovations

E N D
The Australian e-Health Research Centre • Joint Venture between CSIRO and the Queensland Government (2003) • Leading national research facility in ICT for healthcare innovations • Aims to improve the quality and safety of healthcare for individuals and communities through an ICT research program focused on applied outcomes and active adoption by the health system • Multi-disciplinary team ~ 50, including researcher scientists, software engineers and PhD students: • Brisbane • Sydney • Melbourne • Adelaide • Research focus: • Biomedical Imaging • Health Data and Smart Methods Australian e-Health Research Centre
Broadband and health – a great mixture • Health is a knowledge business – communications technologies can deliver better access to knowledge by: bringing expertise to remote locations via tele-medicine, tele-presence and remote training providing enhanced community care and in-home monitoring for the elderly and chronically ill enabling improved techniques for analysis and standardisation medical data. Australian e-Health Research Centre
Tele-medicine, tele-presence and remote training Through the use of telemedicine, all members of society, wherever they are located, can access the same standard of care • Remote check-ups and consultations • Tele-psychology consultations via video link • Remote eye-care – sharing retinal scans and voice • CSIRO RIDES technology –immersive consultation environment • Remote emergency room conferencing • overcoming distance: bringing expertise to rural communities • providing rapid expertise: linking virtual teams across cities • CSIRO VICCU technology – combining video and data • Remote medical training • optimising use of limited skilled trainers • enabling career development for clinicians in rural areas • CSIRO haptic workbench allowed temporal bone surgery training Australian e-Health Research Centre
The Virtual Critical Care Unit (ViCCU®) which permits specialists based at a tertiary referral hospital (Nepean, on the outskirts of Sydney) to guide a team based in a regional hospital (Katoomba) caring for patients in the Emergency Department, using an advanced telemedicine system VICCU Australian e-Health Research Centre
The ECHONET system which assisted bedside assessments, guided echocardiography and case-based education by linking an intensive care unit in north west Tasmania to major ICU and Cardiology Departments at a city hospital. ECHONet Australian e-Health Research Centre
In-home monitoring for the elderly and chronically ill Delivering improved care and decision support • Cardiac rehabilitation using tele-medecine solutions • ambulatory monitoring and remote mentoring using mobile phone • improving access and quality of life for recipients • partnering with Queensland Health / PA hospital Australian e-Health Research Centre
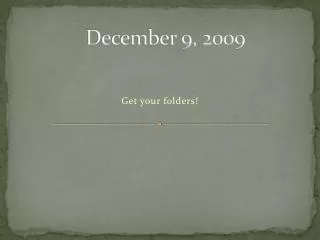
Service Provider Personal devices at home Web portal Health Reports Diary data Measurement data Data display for self management Diary & data synchronisation,photos Server Motivational SMS & VideoRelaxation audio Additional reports uploaded to the system Bluetooth andmanual entry Measurement Devices Mobile Phone Data to server: Community Care Team Treatment & counselling feedback via phone HealthInformation Web-based GUI Diary entries Measurementdata 1) Movement activity and Heart Rate2) Blood Pressure3) Weight scale Diet photos Feedback tools: Video & SMS messages Data in graphical format andhealth report view Videoconference Care Assessment Platform Australian e-Health Research Centre
Sharing medical data Electronic health records provide step gains in care and connectivity, reducing repeat testing and • Improved patient safety • Coordinated care - GPs and hospitals have same information • Reducing repeated testing on admission and discharge • Faster access to data, when and where required • Better quality decision support • Eliminating prescription mix-ups and adverse drug interactions • Easily and reliably view a patient’s (& family) medical history • More effective disease surveillance – eg predicting flu outbreaks • Reduced healthcare costs • reduced labour, storage compared to paper records • reduced cancellations due to missing / delayed test results • consistent data terminology reduces mistakes in patient handover Australian e-Health Research Centre
CRC Surgical Data Link Table CRC Surgical Data Chemotherapy Record Data Chemotherapy Record Data Example Scenario – Integrating data across hospitals Large teaching hospital Private hospital Regional hospital HDI Domain (Remote) HDI Domain(Host) HDI Domain (Remote) Surgical Records Surgical Records Hosp Admin Surgical Records Hosp Admin Surgical Records Chemo Records Hosp Admin Australian e-Health Research Centre
Terminology for data set A Terminology for data set B SNOMED CT SNOMED CT Extensions: using current data • Hypothesis: Can we use SNOMED CT as a base ontology and add “new bits of knowledge” to fully describe data which is collected using other terminologies? Australian e-Health Research Centre
Extracting Meaning from Data- Cancer Staging HISTORY Left upper lobe and partial chest wall. MACROSCOPIC One specimen received.The specimen is labelled "left upper lobe and partial chest wall" and consists of a left upper lobe measuring 155 x 100 x 45 mm. On the lateral aspect of the lung there is attached chest wall and ribs measuring 60 x 60 mm. Deep to this on sectioning, there is a white sclerotic mass measuring 45 x 42 x 40 mm. Surrounding the tumour there is obstructive pneumonitis. No other lesions are identified on sectioning of the lung. The chest wall will be decalcified and a further report will be issued. MICROSCOPIC Sections show a poorly differentiated adenocarcinoma which in most areas comprises sheets of large cells with vesicular nuclei, prominent nucleoli and moderate amounts of eosinophilic cytoplasm. Focally within the tumour there is a cribriform architecture and occasional cells contain mucin vacuoles. Areas of necrosis are present. Tumour invades the overlying thickened pleura and foci of lymphatic permeation are noted within this pleural tissue. Lymphatic invasion is also noted within pulmonary parenchyma. However no metastases are found in peribronchial lymph nodes. No vascular invasion is seen, although thrombus is noted within a vascular space towards the inferior aspect of the tumour. Tumour does not appear to extend up to chest wall structures, but a further report will follow when sections of these are examined. Distant lung parenchyma shows mild centriacinar emphysema. Pathology Report Staging Guidelines Australian e-Health Research Centre
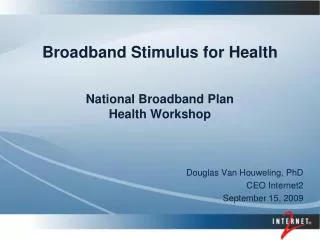
Alzheimer’s Disease Average thickness templates 5 mm 3 mm 0 mm Average NC Average MCI Average AD Australian e-Health Research Centre
Alzheimer’s Disease Building a statistical Atlas of Amyloid deposition Goal: Combining molecular information from PIB PET with anatomical information from MR to generate a computational model of PIB-PET images Statistical analysis of Amyloid deposition in PIB PET images of Alzheimer’s disease, mild cognitive impairment and normal control, consistent with histological analysis Approach: • Standardise subjects brains (using registration to an atlas) • Statistical analysis (PCA) • Classification of new subjects. Evolution of amyloid deposits in AD from autopsy. Adapted from Braak H, Braak E 1997. Courtesy of Department of Nuclear Medicine, Centre for PET, Austin Health, Australia. Australian e-Health Research Centre