Download
1 / 1
10 likes | 73 Views
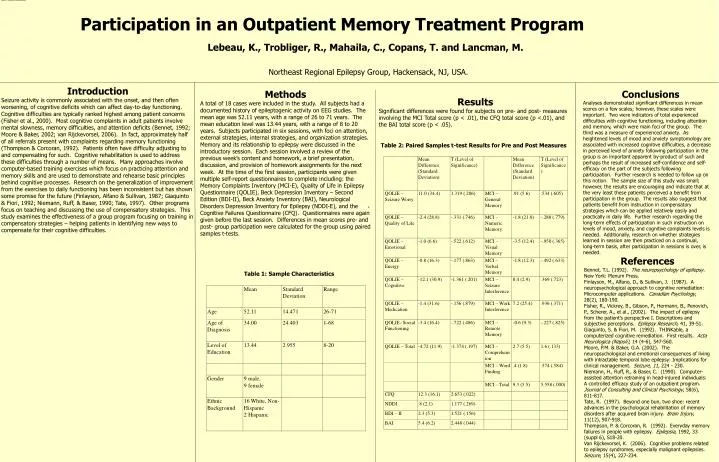
Table 1: Sample Characteristics. Participation in an Outpatient Memory Treatment Program. Lebeau, K., Trobliger, R., Mahaila, C., Copans, T. and Lancman, M. Northeast Regional Epilepsy Group, Hackensack, NJ, USA. Introduction

E N D
Table 1: Sample Characteristics Participation in an Outpatient Memory Treatment Program Lebeau, K., Trobliger, R., Mahaila, C., Copans, T. and Lancman, M. Northeast Regional Epilepsy Group, Hackensack, NJ, USA. • Introduction • Seizure activity is commonly associated with the onset, and then often worsening, of cognitive deficits which can affect day-to-day functioning. Cognitive difficulties are typically ranked highest among patient concerns (Fisher et al., 2000). Most cognitive complaints in adult patients involve mental slowness, memory difficulties, and attention deficits (Bennet, 1992; Moore & Baker, 2002; van Rijckevorsel, 2006). In fact, approximately half of all referrals present with complaints regarding memory functioning (Thompson & Corcoran, 1992). Patients often have difficulty adjusting to and compensating for such. Cognitive rehabilitation is used to address these difficulties through a number of means. Many approaches involve computer-based training exercises which focus on practicing attention and memory skills and are used to demonstrate and rehearse basic principles behind cognitive processes. Research on the generalization of improvement from the exercises to daily functioning has been inconsistent but has shown some promise for the future (Finlayson, Alfano & Sullivan, 1987; Giaquinto & Fiori, 1992; Niemann, Ruff, & Baser, 1990; Tate, 1997). Other programs focus on teaching and discussing the use of compensatory strategies. This study examines the effectiveness of a group program focusing on training in compensatory strategies – helping patients in identifying new ways to compensate for their cognitive difficulties. • Methods • A total of 18 cases were included in the study. All subjects had a documented history of epileptogenic activity on EEG studies. The mean age was 52.11 years, with a range of 26 to 71 years. The mean education level was 13.44 years, with a range of 8 to 20 years. Subjects participated in six sessions, with foci on attention, external strategies, internal strategies, and organization strategies. Memory and its relationship to epilepsy were discussed in the introductory session. Each session involved a review of the previous week’s content and homework, a brief presentation, discussion, and provision of homework assignments for the next week. At the time of the first session, participants were given multiple self-report questionnaires to complete including: the Memory Complaints Inventory (MCI-E), Quality of Life in Epilepsy Questionnaire (QOLIE), Beck Depression Inventory – Second Edition (BDI-II), Beck Anxiety Inventory (BAI), Neurological Disorders Depression Inventory for Epilepsy (NDDI-E), and the Cognitive Failures Questionnaire (CFQ). Questionnaires were again given before the last session. Differences in mean scores pre- and post- group participation were calculated for the group using paired samples t-tests. Conclusions Analyses demonstrated significant differences in mean scores on a few scales; however, these scales were important. Two were indicators of total experienced difficulties with cognitive functioning, including attention and memory, which were main foci of the group. The third was a measure of experienced anxiety. As heightened levels of mood and anxiety symptomology are associated with increased cognitive difficulties, a decrease in perceived level of anxiety following participation in the group is an important apparent by-product of such and perhaps the result of increased self-confidence and self-efficacy on the part of the subjects following participation. Further research is needed to follow up on this notion. The sample size of this study was small; however, the results are encouraging and indicate that at the very least these patients perceived a benefit from participation in the group. The results also suggest that patients benefit from instruction in compensatory strategies which can be applied relatively easily and practically in daily life. Further research regarding the long-term effects of participation in such instruction on levels of mood, anxiety, and cognitive complaints levels is needed. Additionally, research on whether strategies learned in session are then practiced on a continual, long-term basis, after participation in sessions is over, is needed. Results Significant differences were found for subjects on pre- and post- measures involving the MCI Total score (p < .01), the CFQ total score (p <.01), and the BAI total score (p < .05). Table 2: Paired Samples t-test Results for Pre and Post Measures . References Bennet, T.L. (1992). The neuropsychology of epilepsy. New York: Plenum Press. Finlayson, M., Alfano, D., & Sullivan, J. (1987). A neuropsychological approach to cognitive remediation: Microcomputer applications. Canadian Psychology, 28(2), 180-190. Fisher, R., Vickrey, B., Gibson, P., Hermann, B., Penovich, P., Scherer, A., et al., (2002). The impact of epilepsy from the patient’s perspective I. Descriptions and subjective perceptions. Epilepsy Research, 41, 39-51. Giaquinto, S. & Fiori, M. (1992). THINKable, a computerized cognitive remediation. First results. Acta Neurologica (Napoli), 14 (4-6), 547-560. Moore, P.M. & Baker, G.A. (2002). The neuropsychological and emotional consequences of living with intractable temporal lobe epilepsy: Implications for clinical management. Seizure, 11, 224 - 230. Niemann, H., Ruff, R., & Baser, C. (1990). Computer-assisted attention retraining in head-injured individuals: A controlled efficacy study of an outpatient program. Journal of Consulting and Clinical Psychology, 58(6), 811-817. Tate, R. (1997). Beyond one bun, two shoe: recent advances in the psychological rehabilitation of memory disorders after acquired brain injury. Brain Injury, 11(12), 907-918. Thompson, P. & Corcoran, R. (1992). Everyday memory failures in people with epilepsy. Epilepsia, 1992, 33 (suppl 6), S18-20. Van Rijckevorsel, K. (2006). Cognitive problems related to epilepsy syndromes, especially malignant epilepsies. Seizure, 15(4), 227-234. Table 1: Sample Characteristics






