Download
1 / 48
490 likes | 977 Views
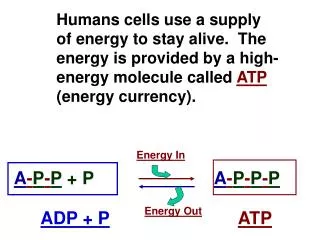
Medical p arasitology. Medical terms you should know Parasite : is a living organism that lives at the expense of its host. Host : the living organism at which the parasite lives on his expense.

E N D
Medical terms you should know Parasite: is a living organism that lives at the expense of its host. Host: the living organism at which the parasite lives on his expense. Parasitism: relationship between two living organisms one gets the benefit (parasite) and the other looses (host). • Parasitology is the science dealing with parasites. • Parasites can be classified into: • Helminthes. • Protozoa. • Arthropods.
As regard to parasite • Obligate parasite is termed when the parasite can live only in a host. • Facultative parasite when it can live both in a host as well as in free form. • Endoparasites parasites that live inside the body. • Ecto-parasites parasites that exist on the body surface. As regard to the host • Definitive (final host): The host that harbors the adult or sexual stages of the parasite. • Intermediate host: The host that harbors the larval or asexual stages of the parasite. • Vector: an arthropod the carries the infective stage of the parasite and can transmit it by active biological sharing in life cycle. • Reservoir hosts: other hosts that harbor the parasite and thus ensure continuity of the parasite's life cycle and act as additional sources of human infection.
General characters of protozoa • Unicellular organisms that are capable of performing whole life functions. • Eukaryotic. • Complex life cycle involving various stages or forms • Reproduction : sexual and asexual • Motility : flagella, cilia, amoeboid movement • These ways of motility are used to divide them into taxonomic groups
Asexual reproduction: Binary fission: longitudinal or transverse. Schizogony : Nucleus undergoes multiple divisions before the cell divides.
Sexual reproduction 1. Gametogony: process often involves production and fusion of gametes. 2. Conjugation and exchange of genetic material between different mating types in Ciliophora (Balantidium coli).
Cyst formation • Encystment of some protozoa is essential for survival outside the body and during the transmision from host to host.
Intestinal protozoa significant to human health include • Entamoebahistolytica (Amebae). • Balantidium coli (Ciliates). • Giardialamblia(Flagellates). • Cryptosporidium parvum and Isospora belli (Sporozoa).
Entamoebahistolytica DiseasesAmebic dysentery and liver abscess. Morphology: it has two form stages Trophozoite: • With the ameboid appearance due to presence of pseudopodia. Cyst: • cysts are spherical with a cyst wall. • 1 to 4 nuclei which are similar to trophozoite. Life cycle There are: no intermediate or reservoir hosts. infective stage: mature cysts. Mode of infection: feco-orally through contaminated food or hands. Clinical Findings # Dysentery. # Amebic abscess Laboratory diagnosis • Finding cysts in the stool. Treatment • Metronidazole (Flagyl) A: Entamoebahistolyticatrophozoite with one ingested red blood cell and one nucleus (circle with inner dotted line represents a red blood cell). B: E. histolytica cyst with four nuclei
Gardialamblia Diseases • Gardiasis= Lambliasis. Morphology Trophozoite: • half pear-shaped organism with 8 flagella and 2 axostyles arranged in a bilateral symmetry. • There are two anteriorly located large suction discs. The cytoplasm contains two nuclei and two parabasal bodies. Cyst: • The cytoplasm contains four nuclei with smooth well-defined wall. Life cycle Definitive host: Man. Infective stage: cyst Mode of infection: ingestion of cysts Clinical finding steatorrhia Laboratory diagnosis • Cysts (constipation) and trophs ( diarrhea) in the stool. TreatmentMetronidazole
Balantidium coli Disease: Balantidiasis. This is a parasite primarily of cows, pigs and horses (zoonotic protozoan). Morphology • Presence of cilia on the cell surface. • Macro- and a micro-nucleus. • Cytostome. Life cycle: • Infective stage: cyst. • Mode of infection: ingestion of cysts in fecal material of farm animals. Symptoms and pathogenesis of balantidiasis are similar to those seen in entamebiasis. However, extra intestinal abscesses are not seen. Diagnosis: • Finding cysts in stool. Treatment: • Metronidazole
Trichomonasvaginalis (a flagellate) Disease: Trichomoniasis Morphology • Trophoziote is the active and infective form, no cyst stage. Life cycle • Infective stage: trophozoites • Infection occurs primarily via sexual contact. Symptoms • In Females withheavy infection: copious foul-smelling yellowish, frothy discharge. Treatment • Metronidazole • Vinegar douche may be useful.
Plasmodium Disease Malaria is caused by four plasmodia: • Plasmodium vivax. • Plasmodium ovale. • Plasmodium malariae. • Plasmodium falciparum. malaria is one of the most common infectious diseases and a leading cause of death.
Life cycle There are two phases in the life cycle: • the sexual cycle in mosquitoes, the final host. • asexual cycle “schizogony”, occurs in humans, the intermediate hosts. • Infective stage: sporozoites • Mode of infection: • Mosquito bites. • Across the placenta. • Blood transfusions. • Intravenous drug abuse. Pathogenesis • Most of the pathologic findings of malaria result from the destruction of red blood cells.
Malaria presents with abrupt onset of fever and chills. • The timing of the fever cycle is 72 hours for P. malariae (quartan malaria) and 48 hours for the other plasmodia (tertian malaria). Malaria caused by P. falciparum is more severethan that caused by other plasmodia because: • It is characterized by infection of more red cells. • Occlusion of the capillaries with aggregates of parasitized red cells leading to: • Cerebral malaria. • Hemoglobinuria "black water fever”. Laboratory Diagnosis Blood films for finding the parasite inside RBcs
Toxoplasma Disease • Toxoplasmagondii causes toxoplasmosis. Life cycle Infective stage • Oocysts in animal stools. • True cysts in meat. • Tachyzoites in blood or transplacentally. Mode of transmission • Ingestion of cysts in uncooked meat or cat feces. • Transplacental transmission: congenital infection of the fetus occurs only when the mother is infected during pregnancy for the 1st time. Clinical Findings • Asymptomatic in immunocompetent adults. • Immunosupressedpatients (e.g., AIDS patients), life-threatening disseminated disease. • Congenital infection. Laboratory Diagnosis • Immunofluorescence assay for IgM antibodyis used. IgM is used to diagnose congenital infection, because IgG can be maternal in origin.
Trypanosoma The genus Trypanosoma includes three major pathogens: Trypanosomacruzi Disease • T. cruzi is the cause of Chagas' disease (American trypanosomiasis). Life cycle • Vector: reduviid bug (cone-nose or kissing bug). • Infective stage: metacyclictrypomastigotes • Mode of transmission: contamination of bite wound with bug’s feces leads to infection.
Clinical Findings • Facial edema and a nodule (chagoma) near the bite. • Fever, lymphadenopathy, and hepatosplenomegaly. • Some patients progress to the chronic form with myocarditis and megacolon. Laboratory Diagnosis • Acute disease :presence of trypomastigotes in films of the patient's blood. • Because the trypomastigotesare not numerous in the blood, other diagnostic methods may be required (1) a stained preparation of a bone marrow aspirate. (2) culture of the organism on special medium.
Trypanosomagambiense & Trypanosomarhodesiense Disease • These organisms cause sleepingsickness (African trypanosomiasis). Life cycle • Vector for both is the tsetse fly. • Infectivestage: metacyclictrypomastigotes. • Mode of transmission: injection of organisms in the saliva of the insect during biting. Clinical Findings • The initial lesion is an indurated skin ulcer ("trypanosomal chancre") at the site of the fly bite. • Enlargement of the posterior cervical lymph nodes (Winterbottom'ssign). • The encephalitis is characterized initially by headache, insomnia and finally coma. Laboratory Diagnosis • Microscopic examination of the blood reveals trypomastigotes.
Leishmania Disease • L. donovani is the cause of kala-azar (visceral leishmaniasis). The life cycle • Vector: sandfly. • Infective stage: metacyclicpromastigotes. • Mode of infection: bite of sand fly.
Visceral leishmaniasis Clinical Findings • Symptoms begin with intermittent fever, weakness, and weight loss. • The disease affect reticuloendothelial system leading to enlargement of the spleen. • Hyperpigmentation of the skin is seen in light-skinned patients (kala-azar means black sickness). • Post kalazar dermal lishmaniod.
Cutaneousleishmaniasis Old world cutaneousleihmaniasis “oriental sore”: charecterized by uler at the site of bite faceor exposed parts of the bodythe lesion heals spontaneously in 1-2 years leaving disfiguring scar. New word cutaneousleishmaniasis • Mucocutaneousleishmaniasis: skin lesions which metastasize to oropharynx after months or years leading to destruction of cartilage. • Checlero’s ulcer: single lesions affecting ears
Laboratory Diagnosis • Diagnosis is usually made by detecting amastigotes in a bone marrow, spleen, or lymph node biopsy or "touch" preparation. Treatment • Pentavalentantimonial drugs. Prevention • Treatment of cases. • Vector control. • Active immunization with living organism from an active ulcer results in life long protection.
3 main classes of medically important helminthes 1. The Nematodes 2. The Trematodes 3. The Cestodes
Trematoda (Flukes) • Hepatic flukes: - Fasciolagigantica. - Fasciola hepatica. • Intestinal flukes: - Heterophyesheterophyes. • Blood flukes: - Schistosomahaematobium. - Schistosomamansoni. • Lung fluke: - Paragonimus
Fasciolagigantica Disease: Fascioliasis, liver rot. Morphology • The adult is a large fleshy worm. • The adult worms live in the bile ducts of herbivorous animals & man. • Fasciolahaptica differs from Fasciolagigantica: - Smaller in size (3 x 1.3 cm). - Intermediate host: Lymnaeatrancatula. Life cycle • Final host: herbivorous animals and human. • Intermediate host:Lymnaeacailliaudi snail • Infective stage: encysted metacercaria. • Mode of infection: ingestion of encysted metacercariain aquatic vegetables (usually leafy plants e.g. lettuce) or in water.
Clinical finding: • Fever • Enlarged tender liver • Biliary colic. • Jaundice. Laboratory diagnosis: Detection of eggs in feces or duodenal aspirate. Treatment: Antiparasitic drugs e.g. Bithional.
Heterophyesheterophyes Morphology: Very small, intestinal flukes. Disease: Heterophyiasis. Life cycle: • Final host: Man & fish eating animals. • Two intermediate hosts: • Pirenellaconica snail . • Bolty & boury fishes. • Infective stage: encyctedmetacercaria. • Mode of infection: eating raw, undercooked or freshly salted fish containing encysted metacercaria. Clinical findings Colicky pain and diarrhea. Egg emboli Laboratory diagnosis Detection of the eggs in faeces. Treatment Antiparasitic drugs, Praziquantel
Schistosoma Disease:Schistosomiasis (Bilharziasis). It differs from other trematodes in : • Separate sexes. • Eggs with spine. • Cercaria is the infective stage. 3 known schistosomes infect humans: • S. haematobium • S. mansoni: • S. japonicum • S.mansoni : mesenteric venules of bowel &, rectum. It causes intestinal schistosomiasisand eggs pass in stool. • S. haematobium: venous plexus of the bladder, ureter & kidneys. It causes urinary schistosomiasisand eggs pass in urine.
Lifecycle • Intermediate hostis a snail • S. heamatobium (Bulinustrancatus) • S. mansoni (Biomphalariaalexandrina). • Infective stage: is the cercaria • Mode of infection: Penetration of the cercaria(which is attracted to man by the body temperature) to skin when water begins to dry. Clinical features Urinary bilhariziasis: terminal haematuria. Intestinal bilhariziasis: dysentery. • Laboratory diagnosis: Detection of eggs in stools or urine. Treatment: Praziquantel.
Taeniasaginata(beef tapeworm) Disease: taeniasissaginata. Morphology: • Has a scolex. • Segmented from 1000-2000 segments. • Immature segments. • Mature segments. • Gravid segments. Life cycle: Definitive host: human. Intermediate host: cattle (beef). Infective stage: Cysticercusbovis. Mode of infection: ingestion of raw or improperly cooked beef containing the cysticercusbovis. • Ingestion of eggs is not infective to human. Clinical finding #Intestinal obstruction#Loss of weight as the parasite consumes much of patient’s food. Diagnosis Detection of the eggs or gravidsegments in stool. T. soliumis the same as T. saginatabut. • Intermediate host is the Pork • Eggs could be infective to human leading to cysticercosis.
Diphyllbothriumlatum (fish tapeworm) Disease: Diphyllobothriasis Morphology • Formed of scolex & 3000-4000 immature & mature segments (no gravid segments). Life cycle • Definitive hosts: man, dogs, cats and other fish-eating animals. • 1st intermediate host: Cyclops • 2nd intermediate host: Fresh water fishes e.g. salmon. • Infective stage is Plerocercoidin infected fish muscles ( the 2nd intermediate host). • Mode of infection: by eating infected fishes either raw or improperly cooked (smoked or pickled). Clinical features • Intestinal symptoms • Macrocytichyperchromic anemia Diagnosis: • Detection of eggs in feces. Treatment: • Antiparasitic drugs.
Hymenolepis nana (Dwarf tapeworm) Disease:hymenolepiasis nana Life cycle: • Adult worms live in the small intestine • Definitive hostsare human, rats & mice More common in children. • Infective stage: egg. • Mode of infection: • Ingestion of eggs through; • Contaminated food. • Autoinfection either internal or external. • Clinical picture • In heavy infection: • Intestinal irritation, enteritis • Nervous manifestations Diagnosis: • Detection of eggs in stool. Peranal swab is more diagnostic. Treatment: • Antiparasitic drugs, praziquantel.
Echinococcusgranulosa (Dog tapeworm) Disease: hydatid cyst disease Morphology: • scolex and only three proglottids, making it one of the smallest tapeworms. • Humans are almost always dead-end intermediate hosts. Clinical features • The cyst acts as a space-occupying lesion, putting pressure on adjacent tissue. • The cyst fluid contains parasite antigens, if the cyst ruptures spontaneously or during trauma or surgical removal, life-threatening anaphylaxis can occur. Diagnosis • Indirect hemagglutination test. • Surgical removal and microscopic examination of cyst contents. • Treatment Treatment • Albendazole with or without surgical removal of the cyst.
Enterobiusvermicularis(pinworm) Disease: pinworm infection (enterobiasis). Life cycle: • Infective stage: Egg. • Mode of infection: ingesting of the worm eggs. • At night, the female migrates from the anus and releases thousands of fertilized eggs on the perianal skin and into the environment. Clinical Findings • Perianalpruritusis the most prominent symptom. Diagnosis • The eggs are recovered from perianal skin by using the Scotch tape technique and can be observed microscopically (Figure 56–3). • Unlike those of other intestinal nematodes, these eggs are not found in the stools. Treatment • Mebendazole . Whole family must take the treatment as it is highly infectious.
Trichuristrichiura(whipworm) Disease: whip worm infection or trichuriasis Life cycle: • Infective stage is emberyonated egg. • Mode of infection: ingesting worm emberyonated eggs in food or water contaminated with human feces. Clinical Findings • Trichuris may cause rectal prolapse in children with heavy infection. Prolapse results from increased peristalsis that occurs in an effort to expel the worms. Laboratory Diagnosis • Diagnosis is based on finding the typical eggs, i.e., barrel-shaped with a plug at each end, in the stool Treatment • Mebendazole is the drug of choice.
Ascarislumbricoides Disease: ascariasis Life cycle: • Infective stage: egg. • Mode of infection: ingesting eggs in food or water contaminated with human feces Clinical Findings • Most infections are asymptomatic • Malnutrition and intestinal obstruction in a heavy worm burden patient. Laboratory Diagnosis • Microscopically by detecting eggs in the stools. Treatment • Both mebendazole and pyrantelpamoate are effective.
Ancylostomaduodenale (hookworm) Disease: Ancylostomiasis. Life cycle: • Infective stage: filariform larvae. • Mode of infection: penetration of the skin by the filariform larvaeonwalking with bared foot on moist soil. Clinical Findings • loss of blood at the site of attachment in the small intestine will lead to microcyticaneamia. Laboratory Diagnosis • Microscopically by finding eggs in the stools. Treatment • Both mebendazole and pyrantelpamoate are effective.
Wuchereria Disease: W. bancroftileads to elephantiasis. • Vector: female mosquito (especially Anopheles and Culex species). • Infective stage: infective larvae. • Mode of infection: Humans are infected when the female mosquito deposits infective larvae on the skin while biting. Clinical Findings • Adult worms in the lymph nodes cause inflammation that eventually obstructs the lymphatic vessels, causing edema. Massive edema of the legs is called elephantiasis. Laboratory Diagnosis • Thick blood smears taken from the patient at night reveal the microfilariae. Treatment • Diethylcarbamazine is effective only against microfilariae; no drug therapy for adult worms is available.