Download
1 / 87
890 likes | 1.2k Views
Female Reproductive System I, Dr Rotimi Adigun. Female Reproductive System Outline I. Cervix Vulva Vagina Uterus. Female Reproductive System Outline. Cervix. Development of transformation zone. Transformation Zone. Significance: Ectropion in young women, normal

E N D
Female Reproductive System Outline I • Cervix • Vulva • Vagina • Uterus
Female Reproductive System Outline • Cervix
Transformation Zone Significance: Ectropion in young women, normal Nabothian cysts because of blockade of endo- cervical glands Transformation zone provides a zone of immature cells which is more vulnerable to infection by HPV.Hence development of CA cervix.
Transformation zone Normal cervix, young adult
Cervicitis • Commonest organism, C.Trachomatis Others: • Ureaplasma urealyticum, T. vaginalis, Candida spp., Neisseria gonorrhoeae, herpes simplex II Clinical: • Leucorrhea • Acute and chronic inflamation • Cervical excitation tenderness(Chandelier test) Herpes simplex in pregnant women may cause fatal neonatal infection.
Cervical Carcinoma • Once the most common cancer in women – now not even in top 10. • Decrease due to Pap test in the last 50 years • At the same time, precursor lesions are increasing (early detection)
Cervical Intraepithelial Neoplasia (CIN) • Precursor to carcinoma • Almost all carcinomas arise in CIN; but not all cases of CIN progress to carcinoma! • Three grades: • CIN I: mild dysplasia (half regress, 20% progress) • CIN II: moderate dysplasia • CIN III: severe dysplasia (30% regress, 70% progress) • The higher the grade, the more likely the lesion will progress to carcinoma
Cervical Carcinoma Current grading system: Two grades. Low grade Squamous intraepithelial lesions ,LSIL(CIN I)..Rx. Observation. High grade Squamous intraepithelial lesion, HSIL(corresponding to CIN II and III)Rx. Biopsy.
normal CIN I CIN II CIN III I Cytology of CIN (Pap smear)
normal CIN I CIN II CIN III “Low-grade dysplasia” “High-gradedysplasia” Cytology of CIN (Pap smear)
Cervical Carcinoma Risk Factors • Early age at first intercourse • Multiple sexual partners • A male partner with multiple previous partners • Persistent infection with “high-risk” HPV(16=60%,18) • Smoking • Immunodeficiency
Cervical Carcinoma and HPV • HPV is detectable in almost all CIN and cancer. • “High-risk” types: • 16, 18, 45, 31 • Found in carcinomas • Integrate into genome, inactivate p53, RB • “Low-risk” types: • 6,11 • Found in condylomas (benign lesions) • Do not integrate into genome
Cervical Carcinoma and HPV • HPVs infect immature basal cells of the squamous epithelium via immature metaplastic squamous cells present at the squamocolumnar junction. • Mature superficial squamous cells that cover the ectocervix, vagina, or vulva are spared. Hence a relatively low frequency of vulvar and penile cancer compared to cancers in d cervix.
Cervical Carcinoma and HPV Pathogenesis: Viral E6 and E7 proteins are critical for the oncogenic effects of HPV. • E6:Inactivation of P53,upregulation of telomerase. • E7: Inactivation of Rb ,up-regulation of cyclin, • The physical state of the virus differs in different lesions, being integrated into the host DNA in cancers, and present as free (episomal) viral DNA in condylomata and most precancerous lesions.
Cervical Carcinoma and HPV • Many women with HPV never develop carcinoma.Hence other factors play a role.(Other co-carcinogens, the immune status of the individual, and hormonal factors)
Invasive Cervical Carcinoma • Most cases are squamous, arising from CIN • Small number are adenocarcinomas • Peak age: 45 (10-15 years after CIN develops!) • Spreads slowly • Most cases are diagnosed early • Mortality is related to stage: • stage 0 (preinvasive): 100% 5 year survival • stage 4: 10% 5 year survival
Cervical Carcinoma • Clinical: • Exophytic - necrotic fungating mass • Ulcerative,sometimes infiltrative tumor • 30-50 years • Irregular vaginal bleeding, post-coital bleeding • Vaginal discharge, • Pyometron due to obstruction. • Rx: Surgery +Radiotherapy.
Vulva Bartholin cyst • Acute infection of the Bartholin glands • N. Gonorheah, E.Coli • Edematous, painful vulva • Treatment :Marsupialization.
Vulva Non-Neoplastic Epithelial Disorders of unknown etiology.(NNED) Old name Leukoplakia(white patch), Two distinct entities; • lichen sclerosus and • (2) squamous cell hyperplasia (old name lichen simplex chronicus)
lichen sclerosus Etiology is unknown • Thinning of the epidermis , superficial hyperkeratosis, and dermal fibrosis with a scant peri-vascular, mononuclear inflammatory cell infiltrate • Smooth, white plaques or papules, the surface resembles parchment. • ?Auto-immune disorder. • Age :commonest in Post –menopausal women. • Slightly increased risk of developing Squamous cell carcinoma in women with symptomatic disease.
SQUAMOUS CELL HYPERPLASIA • Old names , hyperplastic dystrophy, or lichen simplex chronicus • Non- specific condition arising from frequent scratching or rubbing of the vulva • It is marked by epidermal thickening, expansion of the stratum granulosum, and significant surface hyperkeratosis. • Squamous cell metaplasia • Association with malignancy is less compared to lichen sclerosus • May occur with Lichen sclerosus or may be seen around established vulva cancer.
Vulva Condylomataacuminata • Hyperkeratosis ,acanthosis and Koilocytes. • Sexually transmitted infection with HPV 6 and 11 • Not associated with malignancy
Vulva Neoplasms Two group of invasive cancers: • Basaloid and warty carcinomas related to infection with high oncogenic risk HPVs (30% of cases) • keratinizing squamous cell carcinomas, not related to HPV infection (70% of cases) • Basaloid and Warty lesions occur in reproductive age women while the peak age for keratinizing squamous cell carcinoma is 76 years.
Vulva Neoplasms Basaloid and Warty cancers: • Develop from Vulva intraepithelial neoplasms,formerly Bowen disease of the vulva (VIN) • HPV 16 responsible for most lesions • Histology shows tightly packed, immature malignant Squamous cells that resemble cells from the basal layer of the normal epithelium. • Younger age group, reproductive age women.
Vulva Neoplasms keratinizing squamous cell carcinomas • Old ,premenopausal women with history of Lichen sclerosus or squamous cell hyperplasia • No HPV infection • Histology shows malignant squamous cells with prominent keratin pearls. • Chronic epithelial cell irritation is responsible.
Paget disease of the vulva Intra-epithelial proliferation of malignant cells Present as • Pruritic, red, crusted, sharply demarcated, maplike area, occurring usually on the labia majora • Disease is confined to the epidermis (unlike breast paget disease where there is underlying malignancy in nearly 100%) • PAS staining would reveal the presence of PAS positive malignant cells. • Treatment is via wide local excision. Recurrence is frequent. • Lesion may persist for decades but metastases is rare.
Vagina Developmental Anomalies, Vaginal Neoplasm,
Developmental Anomalies Vaginal Adenosis • Remnant of columnar endocervix that extend to the proximal vagina during development. • Small patches of columnar epithelium persist after the normal replacement by squamous epithelium. • Seen is in a small percentage of otherwise normal women • Seen in 35-90% of women exposed to DES(increase risk of clear cell carcinoma) Morphology: Red ,granular areas contrasting with the normal pale-pink vagina mucosa.
Developmental Anomalies • Gartner Duct Cyst • Common • Derived from Wolffian duct rests. • 12-cm fluid filled sub mucosal cysts along the lateral walls of the vagina.
Vaginal Neoplasm, Squamous cell Carcinoma of the Vagina • Primary Carcinoma of the vagina is rare • Virtually all are Squamous cell carcinoma arising following infection with high risk HPV. • Most important risk factor=previous Squamous carcinoma of the cervix or vulva. • Vaginal Intraepithelial Neoplasia is the precursor lesion.
Vaginal Neoplasm, Embryonal Rhabdomyosarcoma: • Sarcoma Bortyroides(grapelike tumor) • 1yr-5 yr • Locally aggressive tumor. Causes death by causing urinary tract obstruction or infiltrating the peritoneum • Histology: small neoplastic cells with oval nuclei with a small protrusion of cytoplasm that resembles tennis racket on one side.
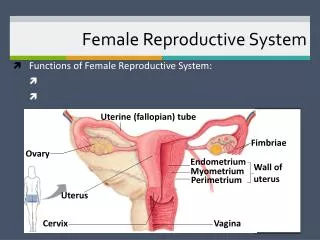
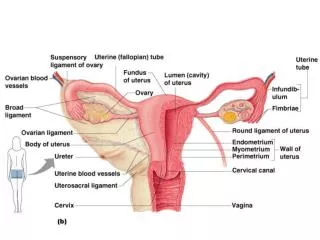
Female Reproductive System Outline • Cervix • Uterus • Endometrial Gland • endometriosis • endometrial hyperplasia • tumors
Uterus Divided into two main parts • Endometrium • Myometrium • Endometrium is a dynamic tissue and the histology changes under hormonal influence.(estrogen, progesterone from the ovary),LH,FSH from the pituitary. • The Myometrium consist of tightly woven smooth muscle fibers. • Endometrial biopsy is done to : “Assess hormonal status, document ovulation and investigate uterine bleeding.
Dysfunction of Menstrual Cycles • Amenorrhea: absence of menstruation • Hypomenorrhea: scanty menstruation • Oligomenorrhea: infrequent menstruation • Polymenorrhea: frequent menstruation • Menorrhagia: excessive menstruation • Metrorrhagia: bleeding between periods • Menometrorrhagia: heavy bleeding during and between menstrual periods
Amenorrhea • Primary amenorrhea • Menarche never occurred • Genetic disorders • Turners syndrome (XO) • Congenital disorders of brain, pituitary, ovary or uterus • Secondary amenorrhea • Cessation of menstrual cycles after a period of regular cycles • Pregnancy
Causes of 2O amenorrhea • CNS or pituitary tumours • Prolactinoma most common • Inhibition of GnRH secretion • Stress, excessive exercise, weight loss • Obstruction of outflow tract • Leiomyoma (fibroid; benign tumour of myometrium) • Asherman’s syndrome (scarring of uterine lining)
Dysfunctional Uterine Bleeding • DUB - uterine bleeding not caused by any underlying organic (structural) abnormality. • Anovulatory cycles are the commonest causes. • DUB is a clinical diagnosis that is made after excluding all organic causes for uterine bleeding such as polyps,fibroids,malignancies.