Download
1 / 22
280 likes | 734 Views
Bone & Joint Infections. Dr. Sudheer Kher Prof & Head Dept of Microbiology Gulf Medical College, Ajman, UAE. Infections of the bones & joints. Both children and adults are affected. Delay and inadequate treatment can result in protracted illness & permanent disability.

E N D
Bone & Joint Infections Dr. Sudheer Kher Prof & Head Dept of Microbiology Gulf Medical College, Ajman, UAE
Infections of the bones & joints • Both children and adults are affected. • Delay and inadequate treatment can result in protracted illness & permanent disability. • Four main diseases are • Osteomyelitis • Septic arthritis • Infection of prosthetic joints • Reactive arthritis Sudheer Kher
Osteomyelitis • Infection of bone and medullary cavity • Tends to recur after treatment • Classification • Basis – Anatomy • Hematogenous • Contiguous focus: with or without vascular insufficiency • Basis – Duration • Acute • Chronic Sudheer Kher
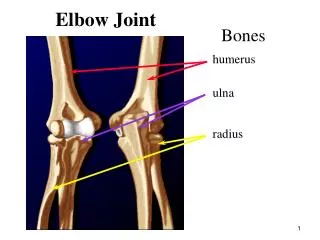
Haematogenous Osteomyelitis • Clinical features – • Children – Usually under 10 Y age, present with acute metaphyseal disease. This region is ideal bacterial ‘seeding’ area: unusual end-artery capillary system forming venous sinusoids of slow-moving blood lacking in phagocytes. • Classical sites – Distal femur, Proximal tibia and proximal humerous. • Presentation – Bone pain, fever, local tenderness. The child is reluctant to move the limb. History of previos trauma may be there. Neonates may not have no localizing signs. Sudheer Kher
Haematogenous Osteomyelitis • Causal organism – Staphylococcus aureus (Most common in all ages) Streptococcus pyogenes Haemophilus influenzae Coliforms Gp B Streptococci in neonates • Source – Not always apparent. Usually septic focus elsewhere e.g. a boil Sudheer Kher
Haematogenous Osteomyelitis • Adults – • Usually secondary to distant focus e.g. infected injection site in IVDU. • Commonly affected sites – • Most common - Vertebrae • Long bones – Diaphysis • In IVDU – Pubic & Clavicular bones often extending into joint cavity. • Presentation – Often non-specific pain and vague symptoms, but can present with acute site specific symptoms. • Causal organisms – Staphylococcus aureus (Most common) Ps. aeruginosa Streptococcus pyogenes Haemophilus influenzae Coliforms Candida sp., Salmonalla sp., Pneumococcus in Sickle Cell Anaemia Sudheer Kher
Contiguous – Focus Osteomyelitis • Infection at any age may follow direct contamination of exposed bones. • Without vascular insufficiency – • After major trauma (compound fracture) • Animal & human bites (Clenched-fist injury) • Puncture wound to calcaneum through soft ‘training shoes’. • Extension of septic arthritis. • Orthopedic surgocal infections: may be device related e.g. fixator sites. • Causal organisms- S. aureus (usually MRSA), coliforms, streptococci and anaerobes. Sudheer Kher
Chronic osteomyelitis • All forms of osteomyelitis can progress to chronicity. • Presentation – • Pain, bone destruction, formation of sequestrum • Discharging sinuses, formation of new bone : involucrum • Brodie’s abscess (late, localised abscess) • Involvement of adjacent joints • Distant spread e.g. endocarditis Sudheer Kher
Chronic osteomyelitis • Causal organisms – • In addition to listed organisms, uncommon causes like • M. tuberculosis • Brucella spp. • Actinomycosis (usually involving dental infections) Sudheer Kher
Lab Diagnosis (osteomyelitis) • Isolation of causal organism & AST • Cultures • Blood cultures – Positive in many hematogenous cases. Several cultures may be necessary. • Pus – • Collected from diseased bone • Needle aspiration • Bone biopsy at open operation • Pus from sinus tract is unreliable Sudheer Kher
Lab Diagnosis (osteomyelitis) • Hematology – • Acute cases – • Polymorphonuclear leukocytosis • Raised ESR • Raised C-reactive proteins • Radiology - Sudheer Kher
Treatment • General – Antibiotic therapy. Empirical for Staph. aureus (flucloxacillin) + Gentamicin if GNB infection suspected. • Surgery – • To drain pus • Remove sequestrum • Obliterate dead space • Restore vascular supply Sudheer Kher
Treatment • Orthopedic procedures • Bone grafting • Stabilization of fractures • Specific treatment • Antibiotic choice – • Basis – Bactericidal activity, Bone penetration, Route of administration (initially parenteral; later switch to oral) • S. aureus – Flucloxacillin + either Gentamicin / Clindamycin / Fusidic acid / Rifampicin • MRSA strains – Vancomycin + Fusidic acid / Rifampicin • Streptococci (Gp A, B or Pneumococci – Penicillin / Clindamycin) Sudheer Kher
Treatment • H. influenzae – Ampicillin / Ciprofloxacin /Ceftriaxone • P. aeruginosa – Ciprofloxacin + Gentamicin • Coliforms, Salmonella - Ciprofloxacin /Ceftriaxone • Anaerobes – Metronidazole or Clindamycin • Tuberculosis, Brucella, Actinomycosis – Specific treatment of the infection. • Note – Treatment must be continued for up to 6 weeks. Sudheer Kher
Septic Arthritis • Infection of the joint space usually seen as • Complication of septicemia in pre-existing joint disease e.g. Rheumatoid arthritis • An extension of osteomyelitis • Infection following intra-articular injection, arthroscopy or orthopedic surgery especially insertion of joint prosthesis. Sudheer Kher
Septic Arthritis • Clinical Features – • Severe pain leading to restriction of movement • Generally single joint involvement – particularly knee • Sudden onset, fever, Swelling, redness over joint • Crippling sequelae common • Causal organsms – • As in Osteomyelitis, Staph aureus most common • Neisseria gonorrhoeae, N. meningitidis, Mycoplasma hominis, Ureaplasma urealyticum, Borrelia burgdorferi Sudheer Kher
Lab Diagnosis (Septic Arthritis) • Examination of Joint fluid • Direct Gram film – • Polymorphs • Bacteria – Presumptive diagnosis & treatment • Culture – Variety of media for causal organsim • Blood Cuture – Positive in 30-60% cases • Culture of specimens from other infected sites – • Throat / Genital tract / Meninges • Sputum/urine in suspected tuberculosis • Serological tests in Brucellosis / Lyme Disease • Molecular Methods for detecting Bacterial DNA in synovial fluid e.g. B. burgdorferi, M. hominis, N. gonorroheae Sudheer Kher
Infection in prosthetic joints • Often organisms of low pathogenecity can infect. • Risk factors – • Rheumatoid arthritis • Diabetes mellitus • Malnutrition • Obesity Sudheer Kher
Infection in prosthetic joints • Clinical features – • Early fulminant, with hematoma or wound sepsis, usually within a month of operation • Delayed indolent low grade painful infection, within one year of surgery Source of Infection – Operation site Patient’s skin / Surgical team / Contact / Theatre air • Late onset septic arthritis –(usually after 2 years) caused by organisms settling in the implant from a transient asymptomatic bacteraemia • Causal Organisms – S. aureus, Coagulase negative Staphylococci, anerobes. Sudheer Kher
Infection in prosthetic joints • Lab diagnosis – • Often impossible due to difficulty in accessing joint • Culture – Perioperative surgical tissue. Culture of sinus track or superficial wound is not recommended. • Hematology – ESR & CRP usually elevated • Radiology Sudheer Kher
Reactive Arthritis • Acute arthritis affecting one or more joints which develops 1-4 weeks after infection of genital or gastrointestinal tracts. • Caused due to immunological mechanism. Joint exudate is sterile. • Forms of reactive arthritis • Post-sexual reactive arthritis – Arthritis + ocular inflammation (Conjunctivitis / Iritis) post non-gonoccal urethritis - Often caused by Chlamydia trachmatis. Almost exclusively seen in men. Reiter’s sundrome – Arthritis + Urethritis + Cojunctivitis Predisposing factors – HLA B 27 – 50% patients Sudheer Kher
Reactive Arthritis • Post-dysenteric reactive arthritis – Arthritis presents after Gastrointestinal infection with Gram-negative bacilli such as shigella, salmonella, campylobacter, yersinia. Affects both men & women. Urethritis and conjunctivitis common features Sudheer Kher