Download
1 / 1
10 likes | 128 Views
Parent-Child Interactions in Behavioral Treatment of Selective Mutism: A Case Study Christina M. Mele Department of Applied Psychology, New York University. RQ2: Child’s Response Rate to Therapist Commands. Method. Diagnosis & Treatment of Selective Mutism. Participants & Setting.

E N D
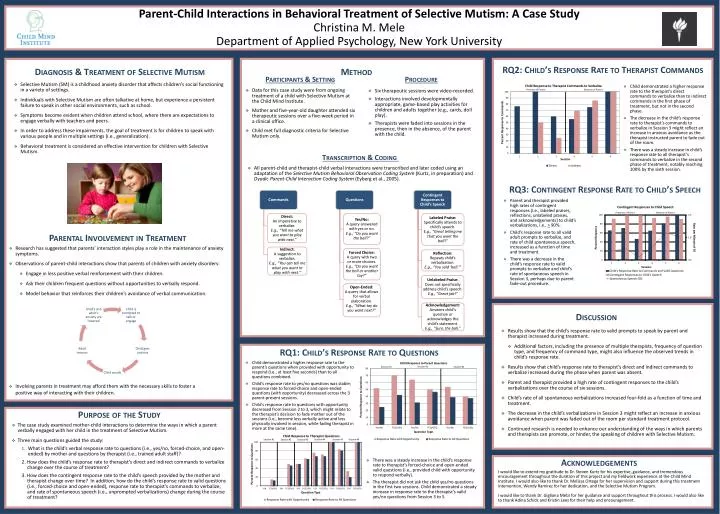
Parent-Child Interactions in Behavioral Treatment of Selective Mutism: A Case StudyChristina M. Mele Department of Applied Psychology, New York University RQ2: Child’s Response Rate to Therapist Commands Method Diagnosis & Treatment of Selective Mutism Participants & Setting Procedure • Selective Mutism (SM) is a childhood anxiety disorder that affects children’s social functioning in a variety of settings. • Individuals with Selective Mutism are often talkative at home, but experience a persistent failure to speak in other social environments, such as school. • Symptoms become evident when children attend school, where there are expectations to engage verbally with teachers and peers. • In order to address these impairments, the goal of treatment is for children to speak with various people and in multiple settings (i.e., generalization). • Behavioral treatment is considered an effective intervention for children with Selective Mutism. • Child demonstrated a higher response rate to the therapist’s direct commands to verbalize than to indirect commands in the first phase of treatment, but not in the second phase. • The decrease in the child’s response rate to therapist’s commands to verbalize in Session 3 might reflect an increase in anxious avoidance as the therapist instructed parent to fade out of the room. • There was a steady increase in child’s response rate to all therapist’s commands to verbalize in the second phase of treatment, notably reaching 100% by the sixth session. • Data for this case study were from ongoing treatment of a child with Selective Mutism at the Child Mind Institute. • Mother and five-year-old daughter attended six therapeutic sessions over a five-week period in a clinical office. • Child met full diagnostic criteria for Selective Mutism only. • Six therapeutic sessions were video-recorded. • Interactions involved developmentally appropriate, game-based play activities for children and adults together (e.g., cards, doll play). • Therapists were faded into sessions in the presence, then in the absence, of the parent with the child. Transcription & Coding • All parent-child and therapist-child verbal interactions were transcribed and later coded using an adaptation of the Selective Mutism Behavioral Observation Coding System (Kurtz, in preparation) and Dyadic Parent-Child Interaction Coding System (Eyberg et al., 2005). RQ3: Contingent Response Rate to Child’s Speech • Parent and therapist provided high rates of contingent responses (i.e., labeled praises, reflections, unlabeled praises, and acknowledgements) to child’s verbalizations, i.e., > 90%. • Child’s response rate to all valid adult prompts to verbalize, and rate of child spontaneous speech, increased as a function of time and treatment. • There was a decrease in the child’s response rate to valid prompts to verbalize and child’s rate of spontaneous speech in Session 3, perhaps due to parent fade-out procedure. Commands Questions Contingent Responses to Child’s Speech Direct:An imperative to verbalize.E.g., “Tell me what you want to play with next.” Yes/No:A query answered with yes or no.E.g., “Do you want the ball?” Labeled Praise:Specifically attends to child’s speech.E.g., “Great telling me that you want the ball!” Parental Involvement in Treatment • Research has suggested that parents’ interaction styles play a role in the maintenance of anxiety symptoms. • Observations of parent-child interactions show that parents of children with anxiety disorders: • Engage in less positive verbal reinforcement with their children. • Ask their children frequent questions without opportunities to verbally respond. • Model behavior that reinforces their children’s avoidance of verbal communication. Indirect:A suggestion to verbalize.E.g., “You can tell me what you want to play with next.” Forced Choice:A query with two or more choices.E.g., “Do you want the ball or another toy?” Reflection:Repeats child’s verbalization.E.g., “You said ‘ball.’” Unlabeled Praise: Does not specifically address child’s speech.E.g., “Great job!” Open-Ended:A query that allows for verbal elaboration.E.g., “What toy do you want next?” Discussion Acknowledgement:Answers child’s question or acknowledges the child’s statement.E.g., “Sure, the ball.” • Results show that the child’s response rate to valid prompts to speak by parent and therapist increased during treatment. • Additional factors, including the presence of multiple therapists, frequency of question type, and frequency of command type, might also influence the observed trends in child’s response rate. • Results show that child’s response rate to therapist’s direct and indirect commands to verbalize increased during the phase when parent was absent. • Parent and therapist provided a high rate of contingent responses to the child’s verbalizations over the course of six sessions. • Child’s rate of all spontaneous verbalizations increased four-fold as a function of time and treatment. • The decrease in the child’s verbalizations in Session 3 might reflect an increase in anxious avoidance when parent was faded out of the room per standard treatment protocol. • Continued research is needed to enhance our understanding of the ways in which parents and therapists can promote, or hinder, the speaking of children with Selective Mutism. RQ1: Child’s Response Rate to Questions • Child demonstrated a higher response rate to the parent’s questions when provided with opportunity to respond (i.e., at least five seconds) than to all questions combined. • Child’s response rate to yes/no questions was stable; response rate to forced-choice and open-ended questions (with opportunity) decreased across the 3 parent-present sessions. • Child’s response rate to questions with opportunity decreased from Session 2 to 3, which might relate to the therapist’s decision to fade mother out of the sessions (i.e., become less verbally active and less physically involved in session, while fading therapist in more at the same time). • Involving parents in treatment may afford them with the necessary skills to foster a positive way of interacting with their children. Purpose of the Study • The case study examined mother-child interactions to determine the ways in which a parent verbally engaged with her child in the treatment of Selective Mutism. • Three main questions guided the study: • What is the child’s verbal response rate to questions (i.e., yes/no, forced-choice, and open-ended) by mother and questions by therapist (i.e., trained adult staff)? 2. How does the child’s response rate to therapist’s direct and indirect commands to verbalize change over the course of treatment? 3. How does the contingent response rate to the child’s speech provided by the mother and therapist change over time? In addition, how do the child’s response rate to valid questions (i.e., forced-choice and open-ended), response rate to therapist’s commands to verbalize, and rate of spontaneous speech (i.e., unprompted verbalizations) change during the course of treatment? • There was a steady increase in the child’s response rate to therapist’s forced-choice and open-ended valid questions (i.e., provided child with opportunity to respond verbally). • The therapist did not ask the child yes/no questions in the first two sessions. Child demonstrated a steady increase in response rate to the therapist’s valid yes/no questions from Session 3 to 5. Acknowledgements I would like to extend my gratitude to Dr. Steven Kurtz for his expertise, guidance, and tremendous encouragement throughout the duration of this project and my fieldwork experience at the Child Mind Institute. I would also like to thank Dr. Melissa Ortega for her supervision and support during this treatment intervention, Wendy Ramirez for her dedication, and the Selective Mutism Program.I would like to thank Dr. Gigliana Melzi for her guidance and support throughout this process. I would also like to thank Adina Schick and Kristin Lees for their help and encouragement.