Download
1 / 47
480 likes | 511 Views
A rare case of IgG4 related disease with pulmonary involvement. Dr. Ram Kommaraju, DO Dr. Jeffrey Carlson, DO 4/26/2018. Objectives. Case presentation Define and describe IgG4-related disease Learn how to suspect and make the diagnosis Brief review of pathogenesis

E N D
A rare case of IgG4 related disease with pulmonary involvement Dr. Ram Kommaraju, DO Dr. Jeffrey Carlson, DO 4/26/2018
Objectives • Case presentation • Define and describe IgG4-related disease • Learn how to suspect and make the diagnosis • Brief review of pathogenesis • Discuss clinical findings and major manifestations • Overview of lung disease patterns and specific clinical presentation • Understand treatment options, risks and benefits • Select literature and guideline review
Statement of Disclosure • We have no real or apparent relevant financial relationships to disclose
Day 1: Initial Presentation • 73yr old WF with shortness of breath • Symptoms for about 1wk before she presented, progressively worsening. Pt also had mild confusion per husband • Home pulse ox showed SaO2 80% on R/A and 84% on 2LNC • Denied any HA, blurry vision, sore throat, CP, abdominal pain, N/V/D, and incontinence. • Associated symptoms included mild lower back pain • Initial VS: BP 113/68, P 99bpm, RR 16bpm, Temp 97.6F, PO 87% 3LNC.
Medical History • PMH • Bladder Tumors • Squamous Cell Cancer Left Lower Extremity s/p graft on 1/2017 • Bilateral Lung Tumors • “Mikulicz Syndrome” • COPD (on 2L oxygen at baseline) • Hypothyroidism • Depression • Urinary Incontinence • PSH • Cholecystectomy, Tumors removed from bladder, Skin Graft of LLE • SH – Patient lives with husband. Could care for herself until summer 2017. Was a nurse growing up. Now retired. 50-pack-yr smoking hx, quit 3mo ago. Denied alcohol and illicit drug use. • FH – Heart Disease, Dementia, Parkinson's Disease
Medications • Respimat Inhaler • Prednisone 20mg Daily • Home Oxygen 2L • Levothyroxine 25MCG • Celexa 40mg Daily • Myrbetriq 25mg Daily • Allergies • Darvocet-N 100, Sulfa, Wellbutrin
Physical Exam General: WDWN. Thin. HEENT: NormocephalicAtraumatic. PERRLA. EOM intact. Mucous membranes dry.Neck: Supple. No masses. Trachea Midline. No lymphadenopathyCardiovascular: S1 S2 present. RRR. No rubs, murmurs or gallops. Respiratory: Respiratory distress noted. Tachypnea. Non-Regular effort and rhythm. Mild crackles, rales, ronchi, and exp. wheezing. Gastrointestinal: Flat. Non-distended. BSX4. Abdomen soft, Non-tender to palpation. No hepatosplenomegaly. Bowel sounds heard in all 4 quadrants.Genitourinary: No foley present.Extremities: No cyanosis clubbing or edema. Bilateral Dorsalis pulses palpated 1+. Pallor of feet bilaterally. Cap refill time 1Skin: No rashes, ulcerations, or lesions. Cool and dry. Neuro: Cranial nerves 2-12 appear intact. No deficits noted. Sensation intact.MSK: Unable to assess stable Gait, ROM, MS +5/5 UE and LE. DTR UE and LE +2/4Psych: AAO x2 patient awake and cooperative. Patient pleasant.
Prior Imaging • 2/5/17 CT Abdomen/Pelvis – 9cm cystic mass with peripheral enhancing elements arising from the lower pelvis in the midline, which is highly suspicious for endometrial or uterine neoplasm. • 2/17/17 TVUS – asymmetric urinary bladder wall thickening suspicious for neoplasm, confirmed by cystoscopy. • 08/2017 Surgical removal of bladder tumor at BRMC • 09/2017 Hospitalized for similar complaints including dyspnea secondary to a possible COPD exacerbation, and also thrombocytosis, leukocytosis. A CT chest was obtained, and she was told to follow-up with Hem/Onc outpatient.
Prior Imaging • 09/09/2017 CT Chest: • Three spiculated masses, two of which are in the apicoposterior segment of the left upper lobe and the third within the superior lingula, suspicious for multifocal lung carcinoma • Subcentimeter pulmonary nodules in the right upper and left lower lobes suspicious for pulmonary metastasis • Mild centrilobular emphysema in the upper lung zones.
Further Imaging and Pathology • Navigational Bronchoscopy • EBUS • Pathology – no malignancy, but IgG4+ plasma cells evident • IgG4-related disease/Mikulicz syndrome diagnosed Prednisone 20mg/day
Day 1: Significant Labs and Imaging • ABG: pH 7.39, PaO2 64, PCO2 36, HCO3 23 • CBC: WBC 59.3; Hb 10.4/Hct 33.6, Plt 564 • CMP: Glu 163, Na+ 131; ALT 78 AST 62 • AlkPhos 149 • T. Bili 1.4 • CT head unremarkable • CT Abdomen/pelvis unremarkable • CT Chest r/o PE - pleural thickening and a left upper lobe spiculated lung nodule
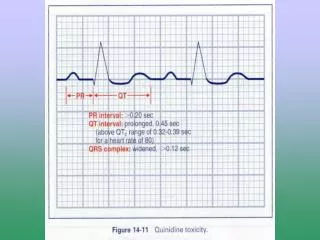
Day 2 • Troponins were elevated at 0.32, with EKG changes noted for diffuse ST elevations. • Patient now on 60L HFNC at 100% sating at 85-87%. • Repeat ABG: pH 7.26, pCO2 55, pO2 72, HCO3 25 • Cardiology was consulted and noted that this was most likely pericarditis and did not wish to pursue any further interventions. • Reversal of Code Status pt intubated • Neurology consult
Day 3 • CBC: WBC 58.3, Hb 7.7/Hct 26.5, Plt 438 • Surgery Consult • VS: HR 93, O2 99%, RR 21, BP 89/52, Temp 97.7F. • Hematology/Oncology Consult • NOT Mikulicz Syndrome but “Probable IgG4 related disease” • Prefer High-Dose Steroid 0.8-1 mg/kg/day rather than medium dose (0.5-0.6mg/kg/day) • Prednisone-reistant, can use Rituximab 1000mg x 2doses
Day 4 • Ventilator Settings: O2 50%, PEEP 6 RR 18 TV 530. • Norepinephrine drip running to maintain pressures. Blood pressure 100/58 with MAP 72. • ABG: pH 7.29, pCO2 52, pO2 70, and HCO3 22. She continued to be intubated and MV. • Repeat CXR – improved aeration in both lung bases • Infectious Disease Consulted • Continue Solu-Medrol with Broad-Spectrum Antibiotics • Rheumatology needed to be involved • Transfer to UVA (Day 5)
Definition • “IgG4-related disease is an immune-mediated fibroinflammatory condition that can affect multiple organs and lead to tumefactive, tissue-destructive lesions and organ failure.” Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med 2012;366:539–51.
Common characteristics • Immune-mediated • Glucocorticoid-responsiveness • Collection of disorders that share pathologic, serologic, and clinical features: • Tumor-like swelling of organs • Lymphoplasmacytic infiltrate with IgG4-positive plasma cells • Variable degrees of fibrosis with “storiform” pattern of histology • Increased serum concentration of IgG4 in 60-70% of patients (>135mg/dL)* *Also seen in Castleman’s disease, Churg-Strauss, and other disorders Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Terms Used to Identify the Disease • IgG4-related disease • IgG4-related systemic disease • IgG4-syndrome • IgG4-associated disease • IgG4-related sclerosing disease • IgG4-related systemic sclerosing disease • IgG4-related autoimmune disease • IgG4-positive multiorgan lymphoproliferative syndrome • Hyper-IgG4 disease • Systemic IgG4-related plasmacytic syndrome • Systemic IgG4-related sclerosing syndrome • Multifocal fibrosclerosis • Multifocal idiopathic fibrosclerosis Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Storiform fibrosis Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
When to Suspect the Diagnosis • Pancreatitis of unknown origin • Sclerosing cholangitis is the most frequent extrapancreatic manifestation of type 1 AIP • Bilateral lacrimal or salivary gland enlargement • Cases of retroperitoneal fibrosis • In patients with orbital pseudotumor or proptosis Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Workup and Diagnostic Considerations • Elevated serum IgG4 level can provide a diagnostic clue • Blood plasmablasts may be a better measure, but are not widely available • Asymptomatic proteinuria may be a sign of renal involvement causing tubulointerstitial nephritis (check C3/C4 levels) • Serum markers of allergic disease including IgE and eosinophils can help narrow the differential • Diagnosed with immunohistochemical staining of tissue sample obtained by surgical resection or core needle biopsy • Consider CT Chest/abdomen/pelvis to grade extent of the disease Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Diagnostic Criteria Diagnostic criteria for IgG4-RD consist of three parts: (1) Clinical examination showing characteristic diffuse/localized swelling or masses in single or multiple organs (2) An elevated serum IgG4 concentration (≥135 mg/dL) (3) Histological examination showing: marked lymphocyte and plasmacyte infiltration and fibrosis; and infiltration of IgG4-positive plasma cells (ratio of IgG4-positive/IgG-positive cells > 40% and an IgG4- positive plasma cell count > 10 per HPF) Umehara H, Okazaki K, Masaki Y, et al. 2012. Comprehensive diagnostic criteria for IgG4-disease, 2011. Mod. Rheumatol. 22:21–30.
Pathogenesis • IgG4-related disease both allergic and autoimmune features • Autoimmune features: • Autoantibodies to lactoferrin/carbonic anhydrase II • Immune-complex deposition • Allergic features: • Increase in Th2 cytokines and increase in serum IgE • Increased incidence of allergic rhinitis and bronchial asthma • Lesions are rich in cytotoxic CD4+ T-cells • Possible mechanism of antigen presentation by T-cells and plasmablasts Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Clinical Findings • Subacute mass (60-90% of cases involve multiple organs) • Cases have been described in nearly all organs of the body • Lymphadenopathy* • Allergy, asthma • Substantial (20-30 lbs/several months) weight loss *Usually not useful for histologic diagnosis Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Major Manifestations • Type 1 (IgG4-related) autoimmune pancreatitis (AIP) • A.k.a. lymphoplasmacytic sclerosing pancreatitis • Characteristic “sausage shape” on CT scan • Salivary gland disease (enlargement or sclerosing sialadenitis) • A.k.a. Mikulicz disease • May present with lacrimal/parotid gland enlargement • Orbital disease • Frequently proptosis secondary to lacrimal gland swelling • May have inflammation, myositis, pseudotumor, dacroadenitis • Retroperitoneal fibrosis • Can cause chronic periaortitis, hydronephrosis • Renal disease may result in tubulointerstitial nephritis Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
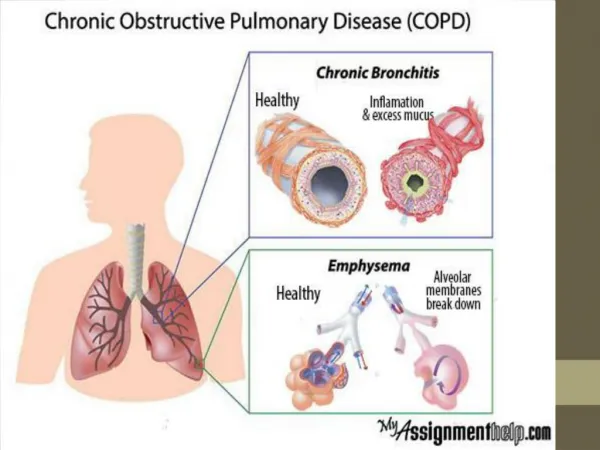
Lung-Specific Manifestations • Isolated lung involvement is rare • Pulmonary involvement can mimic malignancy by presenting radiographically as nodules, masses, pleural lesions, or ground glass opacities (GGOs) • Findings may mimic sarcoidosis • CT may also demonstrate bilateral hilar adenopathy, lung nodules • Bronchoalveolar lavage may yield elevated IgG4 Umehara H, Okazaki K, Masaki Y, et al. 2012. Comprehensive diagnostic criteria for IgG4-disease, 2011. Mod. Rheumatol. 22:21–30. Campbell, Sabrina et al. "Clinical Review of Pulmonary Manifestations of IgG4-related Disease." Ann Am Thorac Soc Vol 11, No 9, pp 1466–1475, Nov 2014 Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Some Clinical Characteristics of IgG4 Pulmonary Disease • May present with cough, hemoptysis, dyspnea, pleurisy, or chest pain • Can cause IgG4-related interstitial pneumonitis • IgG4 respiratory disease can manifest as pulmonary inflammatory pseudotumors • Pseudotumors and interstitial pneumonia can cause pleural thickening visible on chest CT • Histologically, can cause obliterative phlebitis in the lungs Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Obliteratie Phlebitis Case of a 34-year-old man who presented with a mediastinal mass concerning for malignancy. Biopsy revealed IgG4-related disease (IgG4-RD). The image shows obliterative phlebitis, a histopathologic finding that is nearly pathognomonic of IgG4-RD. The vein is clearly outlined, but its lumen is nearly completely replaced with the same inflammatory infiltrate present elsewhere in the lesion. Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Four patterns of lung disease on CT Chest Solid nodular Bronchovascular Alveolar interstitial Round ground-glass opacities Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.) Inoue, Dai et al. "Immunoglobulin G4-related Lung Disease: CT Findings with Pathologic Correlations." Radiology (2009): Vol 251, No 1. pp260-270.
Solid nodular Case of a 71-year-old woman with right lower lung mass having high standardized uptake on PET, subsequently found to be immunoglobulin G4 (IgG4)-related lung disease after resection by VATS and histology showing lymphoplasmacytic infiltration and fibrosis. The lesion presented as a solitary pulmonary nodule with an irregular margin mimicking lung cancer on computed tomography. Okubo, Tetsuyuki et al. “Immunoglobulin G4‐related Disease Presenting as a Pulmonary Nodule with an Irregular Margin.” Respirology Case Reports 5.1 (2017): e00208. PMC. Web. 25 Mar. 2018.
Bronchovascular Case of a 59-year-old man with IgG4-related disease identified as part of a retrospective case review series demonstrates thickening of bronchovascular bundles of the right lung (white arrows). Mild thickening of the interlobular septa is also noted. Inoue, Dai et al. "Immunoglobulin G4-related Lung Disease: CT Findings with Pathologic Correlations." Radiology (2009): Vol 251, No 1. pp260-270.
Alveolar Interstitial Case of a 59-year-old man included as part of a retrospective case review determined to have IgG4-related lung with honeycombing in both lower lobes (black arrows). Bronchiectasis is also observed in both lower lobes (whitearrows). Diffuse GGOs are found in both middle and lower lobes. This patient was initially suspected of having nonspecific interstitial pneumonia on the basis of thin-section chest CT. Inoue, Dai et al. "Immunoglobulin G4-related Lung Disease: CT Findings with Pathologic Correlations." Radiology (2009): Vol 251, No 1. pp260-270.
Round Ground-Glass Opacities (GGOs) Case of a 35-year-old Korean man with IgG4-related lung disease with manifestations similar to those of interstitial lung disease. Chest computed tomography showed diffuse ground glass opacities and rapidly progressive pleural and subpleural fibrosis in both upper lobes. The image shows focal ground glass opacities in the superior segment of the left lower lobe. Ahn, Jee Hwan et al. “A Case of IgG4-Related Lung Disease Presenting as Interstitial Lung Disease.” Tuberculosis and Respiratory Diseases 77.2 (2014): 85–89. PMC. Web. 25 Mar. 2018.
Treatment of IgG4-RD • Symptomatic disease requires urgent treatment • First-line treatment is with systemic glucocorticoids • Patients may require maintenance steroid-therapy • Relapsed disease may require repeat course of glucocorticoids • May consider rituximab in steroid-refractory disease, however, lack of response to glucocorticoids should prompt review of alternate diagnoses Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.)
Retrospective Case Review of IgG4-RLD Treatment, Han et. al. 2017 • 8 patients with IgG4-RLD included 4 men and 4 women, with an average age of (59±4) years (range, 37-74) • Respiratory symptoms of cough, shortness of breath, and expectoration • Extrapulmonary organs were involved in 7 cases • Serum IgG4 levels were elevated in all 8 cases • All were misdiagnosed with other diseases prior to serologic/histologic confirmation of IgG4-RLD Han GJ et al. "IgG4-related lung disease: analysis of 8 cases and literature review." Zhonghua Jie He He Hu Xi Za Zhi. 2017 Mar 12;40(3):193-198.
Retrospective Case Review of IgG4-RLD Treatment, Han et. al. 2017 • Treatments varied: • 3 cases underwent glucocorticoids with immunosuppressant therapy • 2 underwent surgery combined with glucocorticoids • 2 underwent glucocorticoid therapy alone • 1 only underwent surgery • Follow-up time was 4-132 months with 7 remissions, no deaths reported Han GJ et al. "IgG4-related lung disease: analysis of 8 cases and literature review." Zhonghua Jie He He Hu Xi Za Zhi. 2017 Mar 12;40(3):193-198.
International Consensus Guidance Statement on the Management and Treatment of IgG4‐Related Disease (Mar 2015) • International expert panel of 42 members from diverse specialties who have contributed to literature regarding IgG4-RD • Performed comprehensive literature review spanning March 2001 to February 2014, and noted no RCT of treatments for IgG4-RD to date • Used surveys and follow-up discussions to generate consensus statements rergarding treatments • Reported 94% agreement among panel members that biopsy-confirmation is strongly recommended • Also reported 94% agreement that glucocorticoids are first-line therapy Khosroshahi A et al. "International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease." Arthritis and Rheumatology. Vol. 67, No. 7, July 2015, pp 1688–1699
International Consensus Guidance Statement on the Management and Treatment of IgG4‐Related Disease (Mar 2015) • There was 87% consensus that all patients with symptomatic, active IgG4-RD require some form of treatment. • Some experts cited poor tolerance of prolonged high-dose steroid therapy as a rationale for initiating glucocorticoid-sparing therapies early in the treatment course: • Conventional steroid-sparing treatments including Azathioprine (AZA), mycophenolate mofetil (MMF), 6-mercaptopurine (6-MP), methotrexate, tacrolimus, and cyclophosphamide have been used, but poorly studied. • Data from retrospective studies suggest that B cell depletion with rituximab (RTX) is effective • The panel was split requiring the use of combination glucocorticoids and a steroid-sparing immunosuppressive agent from the start of treatment, with only 46% consensus. Khosroshahi A et al. "International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease." Arthritis and Rheumatology. Vol. 67, No. 7, July 2015, pp 1688–1699
International Consensus Guidance Statement on the Management and Treatment of IgG4‐Related Disease (Mar 2015) • The panel was in 94% agreement regarding maintenance therapy following remission induction with glucocorticoids or steroid-sparing treatments. • The panel was in general agreement with 81% consensus that retreatment with glucocorticoids is indicated in patients who relapse off of treatment following successful remission induction. Khosroshahi A et al. "International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease." Arthritis and Rheumatology. Vol. 67, No. 7, July 2015, pp 1688–1699
International Consensus Guidance Statement on the Management and Treatment of IgG4‐Related Disease (Mar 2015) • The panel identified priorities and directions for future research into IgG4-RD management and treatment: Khosroshahi A et al. "International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease." Arthritis and Rheumatology. Vol. 67, No. 7, July 2015, pp 1688–1699
References • Ahn, Jee Hwan et al. “A Case of IgG4-Related Lung Disease Presenting as Interstitial Lung Disease.” Tuberculosis and Respiratory Diseases 77.2 (2014): 85–89. PMC. Web. 25 Mar. 2018. • Campbell, Sabrina et al. "Clinical Review of Pulmonary Manifestations of IgG4-related Disease." Ann Am ThoracSoc Vol 11, No 9, pp 1466–1475, Nov 2014 • Han GJ et al. "IgG4-related lung disease: analysis of 8 cases and literature review." ZhonghuaJie He He Hu Xi ZaZhi. 2017 Mar 12;40(3):193-198. • Inoue, Dai et al. "Immunoglobulin G4-related Lung Disease: CT Findings with Pathologic Correlations." Radiology (2009): Vol 251, No 1. pp260-270. • Khosroshahi A et al. "International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease." Arthritis and Rheumatology. Vol. 67, No. 7, July 2015, pp 1688–1699 • Moutsopoulos HM, Fragoulis GE. Overview of IgG4-related disease. In: UpToDate, Schur PH (Sec Ed), Romain PL (Dep Ed) UpToDate, Waltham, MA. (Accessed on March 25, 2018.) • Okubo, Tetsuyuki et al. “Immunoglobulin G4‐related Disease Presenting as a Pulmonary Nodule with an Irregular Margin.” Respirology Case Reports 5.1 (2017): e00208. PMC. Web. 25 Mar. 2018. • Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med 2012;366:539–51. • Umehara H, Okazaki K, Masaki Y, et al. 2012. Comprehensive diagnostic criteria for IgG4-disease, 2011. Mod. Rheumatol. 22:21–30.