Download

1 / 30
300 likes | 538 Views
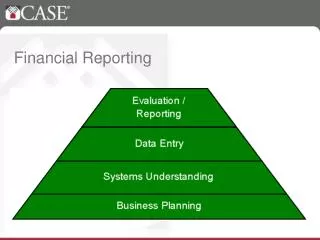
MiPCT Financial Reporting Templates. Carla A. Galligan Consultant. Why Financial Reporting. Financial reporting will ensure accountability for the funds received. Reporting will reconcile revenue collected and expenses. Reporting Templates. There are 4 reporting templates:

E N D
MiPCT Financial Reporting Templates Carla A. Galligan Consultant
Why Financial Reporting • Financial reporting will ensure accountability for the funds received. • Reporting will reconcile revenue collected and expenses.
Reporting Templates • There are 4 reporting templates: Revenue and Membership Care Coordination Practice Transformation Incentive
Basic components of all templates • Revenue (cash collected) • Membership ( corresponds to cash collected) • Expense
Payers included in reporting • Blue Cross Blue Shield of Michigan • Blue Care Network • Medicare • Medicaid Managed Care
Reporting Deadlines • Reports submitted on a quarterly basis for Care Coordination and Practice Transformation . • Incentive reporting is for a 6 month period. • PO/PHO’s will be given 30 days after the quarter end to submit reports . • Due dates: • May 1, 2012 • July 31, 2012 • October 31, 2012 • January 31, 2013 • Data will be submitted electronically. Details on electronic transmission will be finalized by Jan 1, 2012 and will be communicated to PO/PHO’s.
Summary of Payer Membermonths and Revenue • This worksheet purpose is to summarize all payer revenues. • Care Coordination payments are made directly to PO’s for Medicare and Medicaid Managed Care. • Care Coordination payments are made to Practices for BCBSM and BCN. • Practice Transformation payments are made to practices for all payers.
Care Coordination Template • The care coordination template will present all revenue and expenses as outlined in Implementation Plan C.
Care Coordination Expenses • Care Coordination expenses are amounts spent during the reporting period. • Expenses and FTE’s will be cross referenced to Implementation Plan C. • Descriptions of Expenses: Compensation, Overtime, Benefits, Training, Education, Certification, Travel, Meeting Costs and Other (explain).
Care Coordination Expense Documentation Requirements • The PO’s/PHO’s must complete the FTE spreadsheet as support for Care Coordination Expenses. • The FTE spreadsheet purpose is to reconcile compensation and benefit expense as reported . • PO’s/PHO’s will include Implementation C plan FTE data as a data element.
Practice Transformation Template • The Practice Transformation template will present revenue and expenses as outlined in Practice Plan Phase 1.
Practice Transformation Expenses • Practice Transformation expenses are amounts spent during the reporting period. • Expenditures will be cross referenced to Practice Plan Phase 1 item C. Expenditure deviations from the submitted plan are permitted. • Support for FTE’S and Expenses > $5000.00 (single transaction) are required. • Expenses other than Salary and Benefit cost can be assigned on a direct cost or allocation methodology. • The allocation methodology can be used for expenses such as postage, office supplies, telephone etc.. • A column has been added to the templates for designation D – Direct, and A- Allocation. • Support for FTE expenses will be the same as required for Care Coordination. • PO/PHO’s must complete a supplemental report for single disbursements > $5000.00 .
Practice Transformation Support for Single Transaction Expense> $5000.00
Excess Medicaid Managed Care Funds • PO/PHO’s will be allowed to roll forward no more than 20% of Medicaid Managed Care excess of revenue over expense for each reporting module (Care Coordination and Practice Transformation). • An allocation methodology will be used to determine expense by payer using membermonths as the basis for the allocation of expense. • The 20% roll forward will be allowed only if supported by documentation as to why the funds were not expended in the year. • Amounts > 20% will be offset beginning February 2013.
Practice Incentive Reporting • Practice Incentive reporting is defined as all payments received by the PO’s/PHO’s for Medicare and Medicaid Managed Care only. • PO/PHO’s will report funds disbursed to practices. • Reporting requirements are by payer and include: Practice name, Location, Amount, Date. • PO’s/PHO’s are subject to a maximum retention of 20% of the total Incentive dollars received. • The retention of the PO/PHO Incentive dollars >20% may require documentation supporting the dollars retained.
Questions Questions on MiPCT Financial Reporting can be submitted to WWW.MIPCT.ORG contact us.
Clare Tanner and Carol Callaghan Narrative status update
Overview • Narrative Status Update • Detail will vary by quarter • 6 and 12 month report require practice level detail • 3 and 9 months, brief PO- level overview • Avoids duplication of SRD and Quarterly PGIP Progress reports
Narrative Status Update • Content: based on year 1 requirements and priorities • Care Manager hiring progress and barriers • Infrastructure implementation progress across practices • Electronic registry functionality • Care Management documentation • Transition notifications • Opportunity to communicate barriers and successes
Care Management Activity Reporting • Minimum core data: • Number of encounters per care manager, by payer • Will be required beginning third quarter 2012 • Necessary for reporting to participating payers and MDCH • Need to understand PO/practice reporting capacity to minimize burden
Submission • Due dates for quarterly reporting • May 1, 2012 • July 31, 2012 • October 31, 2012 • January 31, 2013 • Submission: email to mipctdemo@michigan.gov