Download
1 / 1
10 likes | 136 Views
A Case Report: Sub-Tenon’s versus General Anaesthesia – A Direct Comparison of a New Anaesthetic Approach for Corneal Graft Surgery. Dr. Birgitt Straub, Dr. Brendan O’Hare, Dr. William Power, Dr. Muhammad Mukhtar Royal Victoria Eye and Ear Hospital, Dublin. Introduction

E N D
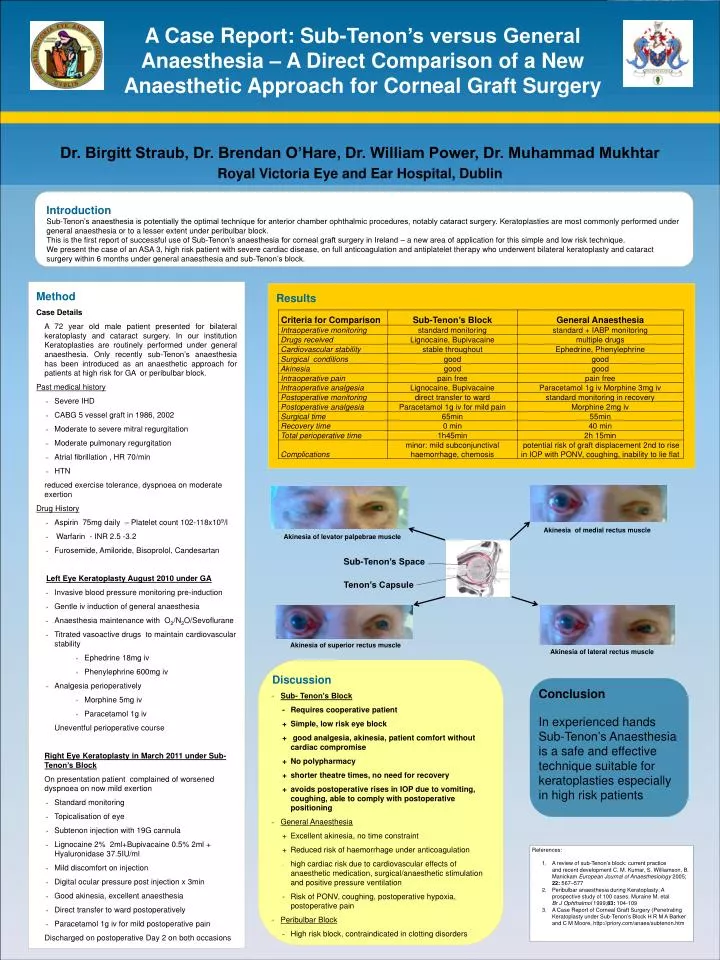
A Case Report: Sub-Tenon’s versus General Anaesthesia – A Direct Comparison of a New Anaesthetic Approach for Corneal Graft Surgery Dr. Birgitt Straub, Dr. Brendan O’Hare, Dr. William Power, Dr. Muhammad Mukhtar Royal Victoria Eye and Ear Hospital, Dublin Introduction Sub-Tenon’s anaesthesia is potentially the optimal technique for anterior chamber ophthalmic procedures, notably cataract surgery. Keratoplasties are most commonly performed under general anaesthesia or to a lesser extent under peribulbar block. This is the first report of successful use of Sub-Tenon’s anaesthesia for corneal graft surgery in Ireland – a new area of application for this simple and low risk technique. We present the case of an ASA 3, high risk patient with severe cardiac disease, on full anticoagulation and antiplatelet therapy who underwent bilateral keratoplasty and cataract surgery within 6 months under general anaesthesia and sub-Tenon’s block. • Method Case Details • A 72 year old male patient presented for bilateral keratoplasty and cataract surgery. In our institution Keratoplasties are routinely performed under general anaesthesia. Only recently sub-Tenon’s anaesthesia has been introduced as an anaesthetic approach for patients at high risk for GA or peribulbar block. • Past medical history • Severe IHD • CABG 5 vessel graft in 1986, 2002 • Moderate to severe mitral regurgitation • Moderate pulmonary regurgitation • Atrial fibrillation , HR 70/min • HTN • reduced exercise tolerance, dyspnoea on moderate exertion • Drug History • Aspirin 75mg daily – Platelet count 102-118x109/l • Warfarin - INR 2.5 -3.2 • Furosemide, Amiloride, Bisoprolol, Candesartan • Left Eye Keratoplasty August 2010 under GA • Invasive blood pressure monitoring pre-induction • Gentle iv induction of general anaesthesia • Anaesthesia maintenance with O2/N2O/Sevoflurane • Titrated vasoactive drugs to maintain cardiovascular stability • Ephedrine 18mg iv • Phenylephrine 600mg iv • Analgesia perioperatively • Morphine 5mg iv • Paracetamol 1g iv • Uneventful perioperative course • Right Eye Keratoplasty in March 2011 under Sub-Tenon’s Block • On presentation patient complained of worsened dyspnoea on now mild exertion • Standard monitoring • Topicalisation of eye • Subtenon injection with 19G cannula • Lignocaine 2% 2ml+Bupivacaine 0.5% 2ml + Hyaluronidase 37.5IU/ml • Mild discomfort on injection • Digital ocular pressure post injection x 3min • Good akinesia, excellent anaesthesia • Direct transfer to ward postoperatively • Paracetamol 1g iv for mild postoperative pain • Discharged on postoperative Day 2 on both occasions Results Akinesia of medial rectus muscle Akinesia of levator palpebrae muscle Sub-Tenon’s Space Tenon’s Capsule Akinesia of superior rectus muscle Akinesia of lateral rectus muscle • Discussion • Sub- Tenon’s Block • - Requires cooperative patient • + Simple, low risk eye block • + good analgesia, akinesia, patient comfort without cardiac compromise • + No polypharmacy • + shorter theatre times, no need for recovery • + avoids postoperative rises in IOP due to vomiting, coughing, able to comply with postoperative positioning • General Anaesthesia • + Excellent akinesia, no time constraint • + Reduced risk of haemorrhage under anticoagulation • high cardiac risk due to cardiovascular effects of anaesthetic medication, surgical/anaesthetic stimulation and positive pressure ventilation • - Risk of PONV, coughing, postoperative hypoxia, postoperative pain • Peribulbar Block • - High risk block, contraindicated in clotting disorders Conclusion In experienced hands Sub-Tenon’s Anaesthesia is a safe and effective technique suitable for keratoplasties especially in high risk patients • References: • A review of sub-Tenon’s block: current practice • and recent development C. M. Kumar, S. Williamson, B. ManickamEuropean Journal of Anaesthesiology 2005; 22: 567–577 • Peribulbar anaesthesia during Keratoplasty: A prospective study of 100 cases. Muraine M. etal Br J Ophthalmol 1999;83:104-109 • A Case Report of Corneal Graft Surgery (Penetrating Keratoplasty under Sub-Tenon’s Block H R M A Barkerand C M Moore, http://priory.com/anaes/subtenon.htm






