Download
1 / 43
430 likes | 672 Views
Adolescents at Risk. Julie S. Downs, PhD. Why Teens Take Risks. Trade off costs (or risks) and benefits Time horizon Probabilistic Conventional wisdom Failure to appreciate risks Perceptions of invulnerability Fischhoff, Parker, Bruine de Bruin, Downs, Palmgren, Dawes, & Manski (2000).

E N D
Adolescents at Risk Julie S. Downs, PhD
Why Teens Take Risks • Trade off costs (or risks) and benefits • Time horizon • Probabilistic • Conventional wisdom • Failure to appreciate risks • Perceptions of invulnerability Fischhoff, Parker, Bruine de Bruin, Downs, Palmgren, Dawes, & Manski (2000)
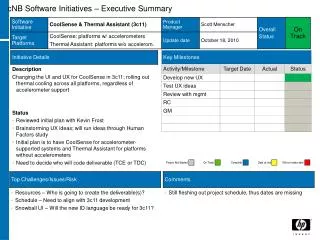
Have a a high school diploma by age 20? Working for pay more than 20 hours/week by age 30? estimate actual 93.4% 84% 92.3% 91% Goals: School and Work
Be the victim of a violent crime in the next year? Be arrested, whether rightly or wrongly, in the next year? estimate actual 14.7% 10% 10.2% <10% Risks: Crime
Die from any cause (crime, illness, accident, and so on) in the next year? Die from any cause (crime, illness, accident, and so on) by age 20? estimate actual 18.6% 0.08% 20.3% 0.4% Risks: Mortality
Teens’ Risk Perceptions • Mildly optimistic about achievements • Greatly overestimate risk of dying young • Implications for risk communications capitalizing on perceived invulnerability • Perceptions follow from communications in non-obvious ways
Optimistic Bias • It’s not just for teenagers • See less risk for ourselves • Even as we overestimate all risks • Feel in control of own outcomes • Know risk of smoking, but… • Less at risk than the “typical smoker” • Think they can avoid risk
Unrealistic Optimism • Some who seem optimistic are realistic • Their health may actually be very good • Some are aware of their high risk • Tie estimates to actual health • Mismatch is often optimistic • These people are particularly resistant to efforts to change behavior
Unrealistic Optimism Unrealistic Optimism “Yeah, but for a fat guy who doesn’t exerciseI’m in pretty good shape.”
Risk Communications • Often ignore common gaps in knowledge and misconceptions Halperin, 1999 • Information chosen for reasons other than needs of target audience Bok & Morales, 1998 • Often repeat well-worn messages that don’t change behavior Crosby & Yarber, 2001
Are We Missing Something? “Despite massive sexual education efforts, more teenage girls are getting pregnant than ever before. Exactly how are all these teens getting pregnant?”
Unhelpful Risk Messages • Attention to very low risks • Exaggeration of risk • Various motivations • Assumption that teens don’t appreciate risk • Desire to control behavior • Liability concerns for products or messages • Little concern about spill-over effects
Overexposure to Warnings • Come to expect warnings • Obvious • Unlikely • Lawyers think it couldn’t hurt
12 fl. oz. (355 ml) DANGER: Harmful or fatal if swallow — FLAMMABLE Read carefully other cautions on the back panel, Child-protective spout Risk Warnings Risk Warnings Harmful if swallowed Warning: thisproduct moveswhen used
Too Many Warnings • Sometimes compensate for poor product design • Better to fix the flaw • Burden on consumer • Desensitize people to real warnings • Lawyers think it couldn’t hurt • But it can hurt!
Risk Estimates • Conventional wisdom • Teens don’t appreciate risk • Need to make sure they are aware • What happens when we distort the risk?
Risks of Body Piercing (Schorzman, Gold, Downs & Murray, 2007)
Inconsistency of information Source may become discredited Discount all information from source Ignore all risk messages Experience may interact with beliefs Undermine all knowledge of domain Draw inappropriate conclusions Problems with Exaggeration
Seek Information After Risk prior to baseline unsafe sex OR=2.15* pregnancy test OR=2.12* condom failure
Draw Reasoned Conclusion prior to baseline at baseline unsafe sex pregnancy test infertility belief OR=3.28* OR=1.22* condom failure misconceptions
Act on Inferences prior to baseline at baseline six months after baseline unsafe sex OR=7.98** pregnancy test infertility belief unsafe sex OR=3.63* misconceptions (Downs, Bruine de Bruin, Murray & Fischhoff, 2004)
Communication of Values • Focus on right vs wrong rather than risk • Avoid problem of wrong information by not providing any • But messages interact with context • Underlying knowledge • Inferences about risk • Inferences about message
Communication of Values Communication of Values
Definition of Abstinence • What does abstinence really mean? • Chastity • Purity • Not having sex • What “counts” as abstinence? • What are abstinent teenagers doing?
Disingenuous Communication • Messages violating known facts • Exaggerated messages did not violate logical relationships • Values-oriented messages did not present logical arguments • May require a network of insincere arguments to sustain
Disingenuous Communication Disingenuous Communication “If a player lands on the ‘Go To Bar’ square he must move directly to the ‘Bar.’ Player does not collect a ‘PINK ELEPHANT’ card. If the player in the ‘Bar’ does not throw a 7 or 11 on his first, second or third turn, he must leave the ‘Bar’ on his third turn by moving the number of squares and taking the number of drinks indicated by the roll of the dice.” —PassOut Rules MINORS FORBIDDEN TO PLAY THIS GAME NOT INTENDED FOR USE WITH ALCOHOLIC BEVERAGES
Reducing High-Risk Behavior • Context affects message impact • Past and future communications • Past and future experiences • Intuitive understanding of domain • As basis for new information • As challenge for changing understanding
Qualitative Barriers • Confidence may not be appropriate • Uncertainty may undermine beliefs • Overconfidence may lead to insensitivity to new information • Conceptual misunderstanding can lead to incorrect inferences • New information may not make sense
Guidance for Content • Focus on well-formulated decision • Gather input • Compare what’s known with what should be known • Evaluate other messages • Develop new messages
Mental Models Approach • Integrated assessment of expertise • Information from target audience • Identify gaps, misconceptions and critical problems in comprehension • Intervention to correct problems • present information relevant to decisions • use nonjudgmental, nonpersuasive tone • Evaluate communication
Teens’ HIV/AIDS Knowledge • High levels of basic knowledge • High confidence in knowledge • Gaps and misconceptions • It only takes once to get HIV • Behaviors are either risky or safe • Protection from Condoms • Know your partner (Bruine de Bruin et al., 2007)
Qualitative Study of Teen Sex • Ignored risk, especially relative risk • Dismissing condoms as not 100% effective • Felt powerless under situational influences • Must avoid normal social interactions • Poor reproductive health knowledge • Knew little of infections other than HIV (Downs et al., 2004)
What Could You Do? • Based on results from interviews • Extensively piloted for comprehension • Nonjudgmental tone maintained • Immediate, non-probabilistic outcomes • Focus on worry as negative outcome • Avoid scare tactics (e.g., fear of AIDS) • Interactive video format
Perceived Risk of Sex • Misconceptions about risk in sexual behavior are common • Risks vary across behaviors • Risks increase cumulatively with more exposures • Risk can be reduced, even if not to zero • Teens may define terms such as abstinence in creative ways
Condom Effectiveness • Misrepresentation of facts • Alleged microscopic “holes” in latex • Alleged link between condom education and sexual behavior • Inappropriate risk comparisons • Dismiss value of relative risk reduction • User vs. method failure rates
Perceived Control Over Sex • Young women may not perceive choices about sexual behavior • Many report sex as normatively driven, without thought about risk • Potential alternative actions • Suggested explicitly in the story • Less risky behaviors are modeled
Girls watching What Could You Do? benefited compared to controls Twice as likely to become abstinent* Condoms failed less than half as often* 45% less likely to report contracting a infection six months later* Fewer tested positive for Chlamydia trachomatis *p<.05 (Downs et al., 2004) Evaluation of Intervention
Conclusions • Consider adolescents’ decision context • Be consistent with real-world information • Mental models interventions • Avoid value judgments • Provide information that fits into the target audience’s existing understanding • Change behavior consistent with shared goals of communicator and audience
References Bruine de Bruin W, Downs JS, Fischhoff B. Adolescents’ thinking about the risks and benefits of sexual behavior. In: Lovett, M. & Shah, P. (Eds.) Thinking with data. Mahwah, NJ: Erlbaum, 2007. Downs JS, Bruine de Bruin W, Murray PJ, Fischhoff B. When “it only takes once” fails: perceived infertility predicts condom use and STI acquisition. Journal of Pediatric and Adolescent Gynecology, 17; 2004:224. Downs JS, Fischhoff B. Parents’ vaccination comprehension and decisions. Internal report to the Centers for Disease Control and Prevention, 2002. Downs JS, Murray PJ, Bruine de Bruin W, Penrose J, Palmgren C, Fischhoff B. Interactive video behavioral intervention to reduce adolescent females' STD risk: A randomized controlled trial, Social Science & Medicine, 59; 2004:1561-72. Fischhoff B, Downs J. Accentuate the relevant. Psychological Science, 8; 1997:154-158. Fischhoff B, Parker A, Bruine de Bruin W, Downs J, Palmgren C, Dawes RM, Manski C. Teen expectations for significant life events. Public Opinion Quarterly, 64; 2000:189-205. Schorzman C, Gold MA, Downs J, Murray PJ. Body piercing attitudes and practices among college students. Journal of the American Osteopathic Association, 107; 2007:432-438..