Download
1 / 45
460 likes | 645 Views
To: President Obama From: Harold Wise, MD, RPSM Founder Re: Beyond Health Care Reform Second Annual Harold Wise Memorial Lecture January 20, 2009 David Kindig MD, PhD University of Wisconsin-Madison School of Medicine and Public Health. Physical

E N D
To: President Obama From: Harold Wise, MD, RPSM Founder Re: Beyond Health Care Reform Second Annual Harold Wise Memorial Lecture January 20, 2009 David Kindig MD, PhD University of Wisconsin-Madison School of Medicine and Public Health
Physical Environment Genetic Endowment Social Environment Individual Behavior Health & Function Disease Health Care Well-Being Prosperity
EVANS AND STODART 1990 “a society that spends so much on health care that it cannot or will not spend adequately on other health enhancing activities may actually be reducing the health of the population”
SOCIOECONOMIC STATUS AND RISK BEHAVIORS • Paula Lantz et al Univ of Mich 2001 • Longitudinal Study 1986-1994…. Americans’ Changing Lives Survey • Four risk behaviors (smoking, BMI, etc) only have modest impact in predicting functional status and self-rated health in low income populations • “risk behaviors are not the dominating mediating mechanism for SES health differences”
THE “FANTASY EQUATION” “at present we but vaguely understand the relative magnitude of the coefficients on the independent variables that would inform specific policies rather than broad directions, even if we are beginning to see the variables themselves more clearly”. G.Stoddart,1995
Rigorous causal relationships Applied research for policy Evidence-based and Evidence-informed policies Policies based on anecdotes and opinions
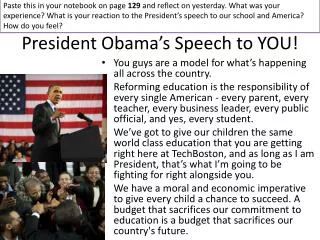
A B C D F Wisconsin Working-Age Adult Mortality Rates (Ages 25-64, rates per 100,000 population) Whites (279) Rural (319) Non-urban (275) Men (367) Suburban (247) Women (225) Milwaukee County (424) Some college (212) High school or less (459) College graduates (188) Native Americans (592) Asians (170) African Americans (624) Best state Minnesota (257) Wisconsin (296) Worst state Mississippi (519)
A B C D F Wisconsin Working-Age Adult Mortality Rates (Ages 25-64, rates per 100,000 population) Whites (279) Rural (319) Non-urban (275) Men (367) Suburban (247) Women (225) Milwaukee County (424) Some college (212) High school or less (459) College graduates (188) Native Americans (592) (279) Asians (170) African Americans (624) (279) Best state Minnesota (257) Wisconsin (296) Worst state Mississippi (519) (277)
A B C D F Wisconsin Working-Age Adult Mortality Rates (Ages 25-64, rates per 100,000 population) Whites (279) Rural (319) Non-urban (275) Men (367) Suburban (247) Women (225) Milwaukee County (424) Some college (212) High school or less (459) College graduates (188) Native Americans (592) Asians (170) African Americans (624) Best state Minnesota (257) Wisconsin (296) Worst state Mississippi (519)
A B C D F Wisconsin Working-Age Adult Mortality Rates (Ages 25-64, rates per 100,000 population) Whites (279) Rural (319) Non-urban (275) Men (367) Suburban (247) (225) Women (225) Milwaukee County (424) Some college (212) High school or less (459) College graduates (188) Native Americans (592) Asians (170) African Americans (624) Best state Minnesota (257) Wisconsin (296) Worst state Mississippi (519) (225)
A B C D F Wisconsin Working-Age Adult Mortality Rates (Ages 25-64, rates per 100,000 population) Whites (279) Rural (319) Non-urban (275) Men (367) Suburban (247) Women (225) Milwaukee County (424) Some college (212) High school or less (459) College graduates (188) Native Americans (592) Asians (170) African Americans (624) Best state Minnesota (257) Wisconsin (296) Worst state Mississippi (519)
A B C D F Wisconsin Working-Age Adult Mortality Rates (Ages 25-64, rates per 100,000 population) Whites (279) Rural (319) Non-urban (275) Men (367) Suburban (247) Women (225) Milwaukee County (424) Some college (212) High school or less (459) (212) College graduates (188) Native Americans (592) Asians (170) African Americans (624) Best state Minnesota (257) Wisconsin (296) Worst state Mississippi (519) (206)
“The fundamental assertion of this book is that population health improvement will not be achieved until appropriate financial incentives are designed for this outcome.” Kindig 1997
Phases of Population Health Improvement Phase 1 Debate, acceptance (1997-2000) and research Phase 2 Outcome based payment (2001-10) for integrated health delivery systems Phase 3 Incorporating the (2011-20) non medical determinants and sectors
“Now is the time to explore possibilities that go beyond medical care determinants and fund demonstration programs…in which community leaders from a variety of sectors can experiment with promising ideas”
BEYOND HEALTHY COMMUNITIES: STRONG MEASURES, REAL RESOURCES “What is required is a coordinated effort across determinants between the public and private sectors, as well as financial resources and incentives to make it work”.
Public Health System Schools Neighborhd. Orgs. Community Centers Employers Transit Faith Instit. Elected Officials Tribal Health Home Health Drug Treatment Non-Profit Organizations Public Health Agency Hospitals Mental Health Fire Civic Groups Nursing Homes Law Enforcement EMS Doctors Corrections Laboratories CHCs
Evans and Stoddart, 2003 “Redirecting resources means redirecting someone’s income…most students of population health cannot confidently answer the question… Well, where would you put the money?”
IF I WERE CZAR, AND HAD TO WORK WITH EXISTING RESOURCES • I would take the 25% of health care expenditures that are thought to be ineffective ($500Billion), and reallocate $100 Billion $300 Billion $100 Billion
TO THE NYT EDITOR “It is encouraging and refreshing that Secretary designate Daschle is considering replacing Medicare fee for service payments with a system that rewards “healthy outcomes” (NYT Jan 9). However, if he means broad health outcomes like life expectancy and infant mortality, his colleagues with responsibility for education, economic development and the environment have as much responsibility as he does.
Social policy is also health policy, and these determinants are as important as health care. Once universal coverage for health care is achieved, perhaps he can become the first Secretary to focus on strong multi-sectoral efforts for real population health improvement.”
Economic Stimulus Package • Prevention block grant: $296 million; Chronic disease programs in general: $545 million; HIV/STD/TB/HBV: $335 million; Environmental health: $60 million; Public health workforce: $30 million; Injury prevention: $50 million; Immunizations: $945 million; Occupational research: $40 million; National Center for Health Statistics: $40 million; Health care associated infections: $150 million; Healthy communities: $500 million; Pandemic preparedness and advanced research and development: $900 million.