Download

1 / 53
550 likes | 675 Views
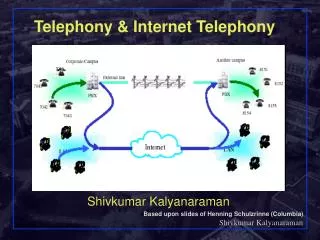
Telephony Bidirectional Interface to Meditech Bed Board. Jean Ferguson Manager, Informatics. Sue MacNeil Director, Food and Environmental Services. Presentation Outline. Profile – Guelph General Hospital Organizational drivers Identifying an opportunity GGH Solution – telephony interface

E N D
Telephony Bidirectional Interface to Meditech Bed Board Jean Ferguson Manager, Informatics Sue MacNeilDirector, Food and Environmental Services
Presentation Outline • Profile – Guelph General Hospital • Organizational drivers • Identifying an opportunity • GGH Solution – telephony interface • Benefits/Outcomes • Next steps
MISSION TOGETHER WITH OUR COMMUNITY AND GUIDED BY OUR VALUES, WE PROVIDE QUALITY, PATIENT-CENTERED HEALTH CAREVALUESCOMPASSION ACCOUNTABILITYRESPECT TEAMWORK Guelph General Hospital Vision We will achieve excellence in everything we do
Information about GGH • GGH is a dynamic, comprehensive acute care facility providing a full range of services to the 180,000 residents of Guelph and Wellington County • GGH is governed by a volunteer Board of Directors • The hospital employs over 1,200 staff • More than 200 Hospital volunteers contribute 1,500 hours of work per month • There are approximately 300 professional staff at GGH including physicians, midwives and dentists
Number of Beds • 22 Critical Care and Step Down • 65 Surgery • 60 Medicine • 14 Obstetrics • 8 Paediatrics Total: 169 beds
Click to edit Master title style Picture Click to edit text
Ontario Healthcare Landscape • The Ministry of Health and Long-Term Care (MoHLT) is working to establish a patient-focused, results-driven, integrated and sustainable publicly funded health system for Ontario based on helping people stay healthy, delivering good care when people need it, and protecting the health system for future generations
MoHLTC Mission and Mandate • Stewardship • Establishing overall strategic direction and provincial priorities • Developing legislation, regulations, standards, policies, and directives to support those strategic directions • Monitoring and reporting on the performance of the health system and the health of Ontarians • Planning for and establishing funding models and levels of funding for the health care system • Ensuring that ministry and system strategic directions and expectations are fulfilled
What is a LHIN? • Local Health Integrated Network • Not-for-profit corporations • Work with local health providers and community members to determine the health service priorities of the region • Plan, integrate and fund local health services, including:
WWLHIN Accountability • Bound by the Local Health System Integration Act 2006 • Accountable to residents Waterloo-Wellington and MoHLTC • Guided by Ministry/LHIN Performance Agreement (MLPA) which defines obligations and responsibilities of the LHIN and MoHLTC • Accountability Agreements between WWLHIN and health service providers of Waterloo Wellington identify: • Responsibilities • Accountabilities • Performance delivery targets
Pay for Results Program (P4R) • Implemented in July 2010 by MoHLTC • Ontario's Pay for Results Program helps hospitals meet specific emergency room (ER) wait time reduction targets • In the first two years overall wait times showed decrease of • 4.7 hours (28%) for patients who require complex medical care or admission to hospital • 1.4 hours (22%) for patients with minor conditions • Hospitals use the funding to ensure more patients are treated within the targets
P4R Indicators • Emergency Room Length of Stay • Date/time of registration or triage to date/time patient left ED • ER LOS Admitted • ER LOS Non-Admitted Complex • ER LOS Non-Admitted Minor • Time to Physician Initial Assessment • Date/time from registration or triage to date/time patient is initially assessed by physician • Time to Inpatient Bed • Date/time from decision to admit to date/time patient left ED
P4R Success Factors • P4R Steering Committee with Senior Team and Physician support and involvement • Recognize impact of inpatient bed availability on Emergency Department • Identify opportunities for improvement • Alignment with LEAN and PIP initiatives • Every Minute Matters Campaign to engage staff GGH has consistently placed in the top ten performers for P4R in Ontario over the past two years
Organizational Drivers • P4R Funding – need to continually improve TAT for patients being admitted from ER to inpatient units to meet targets • Smaller process improvement initiatives identified as a result of broader ED PIP project • “Every Minute Matters” Campaign
Housekeeping Department • 65 staff • 5 shifts (days, evenings, nights + support staff, 1000-1800 and 1200-2000) • Dedicated housekeeping staff in ER 24/7, including breaks • Strategic goal = support patient flow by timely TAT on beds • Trends affecting demands on housekeeping resources: • Increasing # patients requiring isolation – additional cleaning time, additional moves to meet private accommodation and cohorting requirements • Surges in ER creating demands on resources in off-hours • Discharge times fluctuate with changes in surgical programs (ie bariatric program) – need to adjust staffing accordingly • Increase of 9.2% inpatient admissions (2010-2012)
Previous ModelNotification To Housekeeping Of A Dirty Bed • Staff Used: • Bed sheets • Verbal Notification • Phone calls • Pagers
Previous ModelNotification To Unit Staff/BA Of A Clean Bed • Staff Used: • Bedsheets • VerbalNotification • Phonecalls
Issues/Problems • Multiple Processes • Staff confusion, training issues- each unit had their own preferences for communicating when beds were dirty or clean • Wasted time, multiple phone calls/interactions to notify both dirty and clean rooms • Some staff not notified at all – staff notify one person, not the other
Delays In Communication Dirty Bed • Unit staff document on bed sheet; rely on Housekeeper to “see it” • Delays between Bed Allocation being notified and Housekeeping being notified • CleanBed • Housekeeping record time bed cleaned on bed sheet; rely on Unit staff to “see it” • Delays between Bed Allocation being notified and Housekeeping being notified
Trust Issues • Unit staff not reporting discharges = perception that bed is being held to prevent an admission • Unit staff back-timing discharge time on bed sheets appears as though Housekeeper didn’t see or do the bed • Animosity between Housekeepers on multiple shifts regarding workload • Issues between Housekeeping, unit staff, ER and BA when beds are considered to be hidden or held
Fluctuations In Patient Flow • Discharges & transfers batched, often around unit staff shift changes • Multiple beds become available at Housekeeping shift times • Stat beds needed as a result of extended holds • Peaks and valleys in patient flow make it harder to balance/staff the workload • Back-ups in ER followed by ++ admissions difficult to meet TAT’s, P4R targets
Telephony Requirements • Connexall Software / Licensing • Server (Virtual) • Wireless connectivity • Compatible phones for all Housekeeping staff dedicated to inpatient units + 1 RP (Spectralink) • Meditech bidirectional interface • Interface Engine (MDI Solutions)
Step 1 – Entry Of Patient Discharge/Transfer in Room 414-1 On Bed Board • Discharge/transfer of patient in Rm 414-1 activates DIRTY bed status on Bed Board • Discharge/transfer entry on screen includes isolation status, stat bed and whether cleaning required
Step 2 – HL7 Message From Meditech To Spectralink Phone • Message and ring come through on phone indicating Bed 414-1 needs to be cleaned • Stat beds can be identified in message • Isolation status noted, indicating type of cleaning required
Step 3 – Housekeeper acknowledges bed to be cleaned • Housekeeper acknowledges message by pressing green button on left • Bed board updated to “Cleaning In Progress” • Option also to escalate bed to RP by pressing green button on right
Step 4 – Housekeeper cleans bed • Bed added to work assignment; Housekeeper can review bed log on phone • Housekeeper may assign bed verbally to staff who are supporting their unit with discharges; staff let Housekeeper know when they are done • Beds cleaned in order of priority • Bed Board shows Cleaning In Progress
Step 5 – Bed Clean HL7 Message Entered By Housekeeper • Housekeeper chooses bed from list and then chooses custom option on phone to send clean message back to Bed Board
Step 6 – Message Confirmation Of Clean Bed • Message appears on phone confirming status update on Bed Board
Step 7 – Bed Board Updated To Clean Status • Bed Board now shows 414-1 as CLEAN, ready for new admission
Key Steps/DecisionsMapping Beds To Phones Days: • Messages directed to companion phones carried by staff on each unit from 0800-1600 daily • Unit staff responsible for assigning and completing clean message entries for beds on their unit • Option to escalate beds to RP under special circumstances (stat beds, off the unit) during the day • Escalate any beds not yet cleaned at end of shift Evenings/Nights: • Messages directed to one phone from 1600 – 0800 daily • RP (lead) responsible for assigning and completing clean message entries for beds on their shift • Messages (ie dirty beds) stay on phone at shift change times (2400 hrs, 0800)
Key Steps/Decisions Mapping escalation steps in event of no response (ie phone failure, dead zones, misplaced phone) • Housekeeper - if no response (ie ACK) after 5 min - one repeat alert/message - still no response after 5 min - escalate to RP • RP - no response after 5 min - one repeat alert/message - still no response after 5 min - escalate to ER Housekeeping phone • ER Housekeeper - no response after 5 min - retry indefinitely every 5 min * RP = responsible person (lead)
Key Steps/Decisions Delays In Entering CLEAN Message • Potential for delay in cleaning due to volume, 2 step-cleaning and not requesting support • Housekeeper may forget to enter CLEAN message If bed not cleaned within 2 hours message/alert escalates to RP to further assess situation
KeySteps/Decisions Message Details • Unit & bed # • Isolation status • Stat • SWAP bed Isolation Status C Contact CP Contact Plus D Droplet DC Droplet Contact A Airborne AC Airborne
KeySteps/Decisions Coordination With Bed Support Staff • Support staff must coordinate cleaning completion with primary Housekeeper (or RP on evenings) • Challenge during shift changes when beds being escalated to RP yet may be in progress of being cleaned Managing Breaks & Meetings • Decision made that staff not required to respond to calls during breaks but most do as only acknowledgement required (unless stat bed, in which case cleaning would be escalated to RP)
Key Steps/Decisions Downtime • Manual system (old process) utilized if interface down (ie phone calls, pagers, bed sheets) • Pagers used if phones down
Benefits & Outcomes • TAT’s from ER to admission improved • Eliminated all delays between discharge/transfer of patient in system Housekeeping notification • Supported P4R funding
Benefits & Outcomes • Process improvements – clear/automated process for communication between Unit Staff, Bed Allocation & Housekeeper • Improved staff relationships – trust, accountability • Better tracking method for beds needing to be cleaned on a shift • Ability to accurately identify isolation status and therefore type of cleaning at time of notification
Benefits & Outcomes • Opportunity to identify other processes that affect patient flow, patient safety • Infection control risks identified related to bed transfers occurring without cleaning • Manual daily updates of Bed Board unrelated to discharges/transfers risk of errors • Entering “No Clean” when in fact cleaning required
Benefits & Outcomes • Improved workflow, less batching • Fewer stat calls Graph correlates with actual Housekeeping telephony notifications able to plan/adjust staffing accordingly
Reports • Reports provide statistics regarding number and type of cleanings, TAT’s for cleaning • Reports provide ability to investigate concerns regarding delays in admissions
Next Steps Reduce delays in discharge/transfer entries into Meditech = human factor
Ongoing Staff Education • Unit staff – appropriate, timely entries • Housekeeping staff – CLEAN entries to consistently be made 5 minutes before bed is cleaned • Appropriate escalation relative to workload • Continue to review reports to identify patient safety issues requiring education and follow-up
Future Enhancements • Bed Board access on units • Potential applications in outpatient locations • Ability to escalate beds to support staff (requires additional phones and updates to software)