Download
1 / 23
240 likes | 366 Views
IGRT Prostate – the ADHB experience. Nicola Gordon Imaging Specialist RT ADHB. A little history…. 2009 – Orthogonal EPIs #1-3 and weekly – Radiation Oncologists reviewed images 2010 – Introduction of fiducial markers for daily IGRT and RT led image review began

E N D
IGRT Prostate – the ADHB experience Nicola Gordon Imaging Specialist RT ADHB
A little history… • 2009 – Orthogonal EPIs #1-3 and weekly – Radiation Oncologists reviewed images • 2010 – Introduction of fiducial markers for daily IGRT and RT led image review began • Late 2010 – first CBCT capable Linac went clinical – CBCT used for some trial patients • 2011 – began using CBCT to monitor bowel and bladder status on a weekly basis • Mid 2012 – started using VMAT routinely
Evolution of process • CBCT then kV imaging #1-3 & weekly • kV then CBCT #1-3 & weekly • Patients asking if it was a scan day • General lack of understanding from patients • kV then CBCT daily
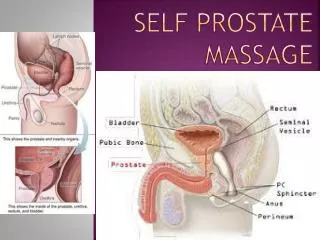
Bladder filling decision rule • 50Gy Isodose curve (maroon) used as minimum bladder filling point.
Rectal filling. • If fiducial match fit was good on kV imaging then treatment continued, with CBCT only for feedback. • If fiducial match fit was not acceptable then the CBCT was used to assess why.
But… • 2 imaging modalities in each fraction for fiducial patients • goes against ALARA principle • Time an issue – increased risk of intrafraction motion. • Effectively soft tissue matching even with fiducials
Soft tissue matching • Some inappropriate fiducial positioning • Patients who were not suitable for fiducials • Prostate Bed patients had soft tissue matching • Consultants preferred fiducials for the majority of patients
Asking our colleagues… • 5 departments use Elekta XVI to match to fiducials on CBCT daily • 1 department using Elekta XVI to match soft tissue on CBCT daily • 1 department using Siemens to match soft tissue on CBCT daily • 2 departments using Varian/ARIA to match to soft tissue on CBCT daily • 5 departments using Varian/ARIA to match to fiducials on kV daily • 1 department using Varian/ARIA to match to fiducials on CBCT #1-3 and weekly and using kV on the other fractions.
Using CBCT to match fiducials • Varian OBI gives only couch corrections that can be applied • Matches done without rotation so need to be ‘best fit’ • If unable to align all 3 fiducials there is probably a reason!
How to visualise Fiducial Contour Colour Blend
Automatch settings. • Bounding Box to cover PTV then use Intensity range and structure VOI of the PTV for automatch.
The process as it stands now • Automatch • Manual adjustment as required • Fiducial match fit • Decision to treat based on bladder and bowel filling • Dose escalation to 78 Gy
Rectum should not be displaced more than 1cm anteriorly into the PTV contour. Current Rectum Decision Rules
Rectum decision rules Before: 28 Minutes later:
Other initiatives • Updated (simplified) Dietary Advice • Weekly MDT ‘On Treatment Chart Round’ • Interventions such as ‘tubing’ • MOODLEs
Time… Post Treatment CBCT study: • Prostate VMAT with Fiducials 6 Min • Prostate VMAT without Fiducials 7.5 Min • Prostate Bed VMAT 6.94 Min • Prostate IMRT (Soft Tissue Match) 12.94 Min
Intra-Fraction Movement - Range • Fiducials: -0.7 to +0.6 (max -0.7 vrt) • Non Fiducials: -0.4 to +0.2 (max -0.4 vrt) • Prostate Bed: -0.5 to +0.5 (max -0.5 vrt) • Prostate IMRT (longer treatment time): -0.3 to +0.4, (max +0.4 - lng)
Moving forwards… • No more fiducial markers! • Finish Accuracy Study • Look at toxicity scores
Thanks • Helen McCabe and the team on MV4 for all their help with Data collection and feedback • Sheonagh Nielson • Rob Lane • All those who responded to the questions we sent out
References • Moseley DJ. White EA. Wiltshire KL. Rosewall T. Sharpe MB. Siewerdsen JH. Bissonnette JP. Gospodarowicz M. Warde P. Catton CN. Jaffray DA. Comparison of localization performance with implanted fiducial markers and cone-beam computed tomography for on-line image-guided radiotherapy of the prostate. International Journal of Radiation Oncology, Biology, Physics. 67(3):942-53, 2007 Mar 1. • Lazos et al, (2012) http://astro2012.abstractsnet.com/handouts/011498_Shifts_Study_ASTRO2012_Poster.pdf • Shi W. Li JG. Zlotecki RA. Yeung A. Newlin H. PaltaJ. Liu C. Chvetsov AV. Olivier K; Evaluation of kV Cone-Beam CT Performance for Prostate IGRTAmerican Journal of Clinical Oncology. 34(1):16-21, 2011 Feb. • NHS (UK) National Cancer Action Team National Radiotherapy Implementation Group Report on IGRT – Guidance for Implementation and Use, August 2012 – Section 18.5