Download
1 / 23
230 likes | 482 Views
Ventricular Assist Devices. Brian Schwartz, CCP February 25, 2003. Criteria for Ventricular Assist Devices. Cardiac Index < 2.0 L/m2/min SVR > 2,100 dyn/sec/cm2 Systolic Pressure < 80 mmHg Atrial Pressure > 20 mmHg Assisted (diuretics) Urine Output < 20 ml/hr Metabolic Acidosis.

E N D
Ventricular Assist Devices Brian Schwartz, CCP February 25, 2003
Criteria for Ventricular Assist Devices • Cardiac Index < 2.0 L/m2/min • SVR > 2,100 dyn/sec/cm2 • Systolic Pressure < 80 mmHg • Atrial Pressure > 20 mmHg • Assisted (diuretics) Urine Output < 20 ml/hr • Metabolic Acidosis
Criteria for Ventricular Assist Devices • Failure to separate from CPB • Irreversible cardiac injury
Short Term Support • Cardiopulmonary bypass Resuscitation • 15 % survival rate • Immediately able to support patient • Need to fully heparinize patient • CPR • Provides support temporarily
Devices Used to Assist the Ventricle(Moderate Setting) • Intra-aortic balloon pump • Cardiopulmonary Support (CPS) • Centrifugal Pump “Bio-Head” • Abiomed (BVS-5000) Bi-Vad
Intra-aortic Balloon Pumps • The least complicated means of circulatory assistance • Effects of IABP • Augmentation of Diastolic Pressure • Decrease Afterload • Decrease myocardial oxygen consumption • Augments C.O. by 10% (500-800 cc/min) • Relatively inexpensive
Intra-aortic Balloon Pumps(Indications) • Cardiogenic shock following MI • Unstable Angina • Left Main Disease • Ventricular Dysrhythmias • Septic Shock
Intra-aortic Balloon Pumps(Contraindications) • AI • Aortic Aneurysm • Severe Femoral Disease
Cardiopulmonary Support (CPS) • Percutaneous insertion • Need oxygenator and heat exchanger • Cannulate both femoral artery and femoral vein • Needs continuous monitoring, therefore very labor intensive • Maximum support…48 hours
Centrifugal Pump • Easy to prime and set up • Requires continuous monitoring • Kinetic assisted venous drainage • ACT’s around 180-200 seconds • Moderate cost
Abiomed • Quick set-up • Minimal bedside monitoring • Supports large children and adults • Flow rates up to 5 L/Min • Maximum use….1 week • Patients are not mobile • High cost
Long Term Devices for Ventricular Support • TCI ( Heartmate IP 1000) Pneumatic • LVAD only • TCI (VE) Vented Electric • LVAD only • Novacor (N 100P) Electric • LVAD only • Thoratec Pneumatic • LVAD, RVAD, Bi-VAD
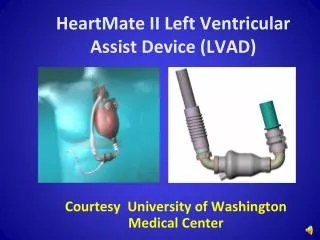
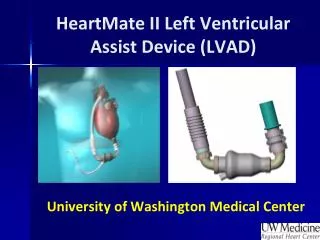
Heartmate Pneumatic LVAD • Allows blood flows to exceed 10 liters per minute • Inserted during CPB • Minimum BSA required…1.7 • Very costly to insert
Heartmate Vented Electric LVAD • Allows flows exceeding 10 liters • Need CPB for placement • BSA requirement…greater than 1.7 • Patients are able to go home • Minimal anti-coagulation • High cost
Total Artificial Heart • CardioWest ( C-70 ) Pneumatic total artificial heart • C.O. is approximately 7.0 L/M • BSA>1.7 • Need CPB for implant • Native heart not excised • Need Anti-coagulation • Patient in-house but mobile
Total Artificial Heart • Abiomed’s total artificial heart • Still in clinical trials • First patient lasted several months on device • If successful, will save hundreds of thousands of live because there will be no waiting like the transplant list
Signs indicating Left Ventricular Failure • Decreased contractility • Elevated left ventricular filling pressures • Elevated pulmonary capillary wedge pressures • Decrease pulmonary oxygenation
Signs of Right Ventricular Failure • Cardiac Index less than 1.8 L/min/m2 • Aortic pressure less than 90 mmHg • Atrial pressure greater than 20 mmHg • Pulmonary capillary wedge pressure less than 10 mmHg
Cannulation sites for LVAD’s • Inlet • Left atrium • Left ventricle • Left superior pulmonary vein • Outlet • Aorta
Cannulation sites for RVAD’s • Inlet • Right atrium • Outlet • Pulmonary artery
Heparin Management in Patients with VAD’s • ACT’s are maintained around 180-200 seconds…as long as the cardiac output is above three liters per minute • ACT’s are maintained above 300 seconds while the cardiac output is below three liters per minute • WHEN IS THIS IMPORTANT???????
Discontinuing a VAD • If possible, the heart is allowed to rest for 48-72 hours • Weaning the patient off the assist devices is then performed. ( Patient needs to have a native C.I. of at least 2.2 L/min/m2) • ACT’s are increased to compensate for the low flows • If the patient tolerates the low flows, he/she is separated from the assist devices and the cannulae are removed
VAD Protocol for Your Institution • Know your protocol • Know your equipment • Be able to predict those patients at risk • Be able to prime in an orderly fashion • Be prepared to assist the surgeons • Help educate all staff working with the patient