Download
1 / 35
350 likes | 355 Views
fffff rgergeger

E N D
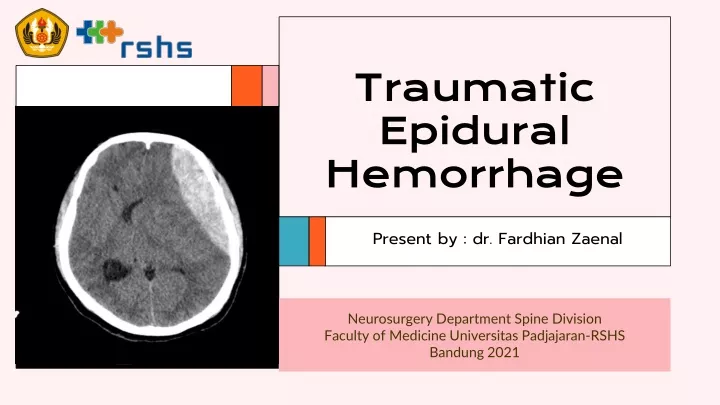
Traumatic Epidural Hemorrhage Present by : dr. FardhianZaenal Neurosurgery Department Spine Division Faculty of Medicine UniversitasPadjajaran-RSHS Bandung 2021
Anatomy of Skull Skull consist of Frontal bone, ethmoid bone, sphenoid bone, temporal bone, parietal, and occipital bone. Rhoton : Atlas of Head, Neck , and Brain.
Anatomy of Skull : lateral view Rhoton : Atlas of Head, Neck , and Brain.
Anatomy of Skull : posterior view Rhoton : Atlas of Head, Neck , and Brain.
Anatomy of Skull : superior view Rhoton : Atlas of Head, Neck , and Brain.
Anatomy of Skull Anatomical notes Superior and inferior view of skull Rhoton : Atlas of Head, Neck , and Brain.
ANATOMY OF SKULL 3 layers of calvaria : Outer table, Diploe, Inner Table Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Epidural Hemorrhage • Epidural hemorrhage or later being a hematoma (EDH) is an extra-axial collection of blood within the potential space between the outer layer of the dura mater and the inner table of the skull. • It is confined by the lateral sutures (especially the coronal sutures) where the dura inserts. • It is a life-threatening condition, which may require immediate intervention and can be associated with significant morbidity and mortality if left untreated. • Rapid diagnosis and evacuation are important for a good outcome Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Etiology : Non-traumatic mechanisms include the following: • Infection/Abscess • Coagulopathy • Hemorrhagic Tumors • Vascular Malformations Majority of cases related to a traumatic mechanism are a result of head injury due to motor vehicle collisions, physical assaults, or accidental falls Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Epidemiology : • Incidence of epidural hematoma (EDH): 1% of head trauma admissions (which is ≈ 50% the incidence of acute subdurals). • Ratio of male:female = 4:1. • Usually occurs in young adults, and is rare before age 2 yrs or after age 60 (perhaps because the dura is more adherent to the inner table in these groups) • Source of bleeding: 85% = arterial bleeding (the middle meningeal artery is the most common source of middle fossa EDHs). • 70% occur laterally over the hemispheres with their epicenter at the pterion, the rest occur in the frontal, occipital, and posterior fossa (5–10% each) Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Pathophysiology of EDH Most epidural hematomas result from arterial bleeding from a branch of the middle meningeal artery. The anterior meningeal artery or dural arteriovenous (AV) fistula at the vertex may be involved Arterial Injury Venous Injury Up to 10% of EDHs are due to venous bleeding following the laceration of a dural venous sinus. In adults, up to 75% of EDHs occur in the temporal region. However, in children, they occur with similar frequency in the temporal, occipital, frontal, and posterior fossa regions.A skull fracture is present in the majority of patients with EDH. These hematomas often present beneath a fracture of the squamous part of the temporal bone. Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Classification based on Radiographic Progression • Type I: Acute; occurs on day 1 and associated with a “swirl” of un-clotted blood • Type II: Subacute occurring between days 2 to 4 and usually solid • Type III: Chronic occurring between days 7 to 20; mixed or lucent appearance with contrast enhancement Acute EDH. (a) Non-contrast axial CT shows a characteristic hyperdense, homogeneous, biconvex left temporal extra-axial collection (arrow). (b) An adjacent axial CT slice, displayed in bone window, reveals associated pneumocephalus and a linear non-displaced fracture of the left temporal bone (arrow) Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Classification based on Radiographic Progression Subacute EDH on MRI. Proton density-weighted axial MR image shows a thin dark line (horizontal arrows) displaced by the extra-axial collection, indicating the epidural location of the hematoma. A contrecoup left orbitofrontal contusion is also evident (asterisk) Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Classification based on Radiographic Progression EDH “swirl sign.” (a) Axial CT image shows low attenuation areas (arrow) within a left frontotemporal heterogeneous acute EDH. The heterogeneous density within this EDH is secondary to mixing of hyperacute (low attenuation) with acute (high attenuation) blood. (b) Axial CT image from another patient, performed following decompressive craniectomy, demonstrates right external herniation, left-to-right subfalcine herniation (arrows), and formation of a contralateral, heterogeneous EDH Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Classification based on Radiographic Progression Venous EDH. (a) Axial CT image shows a biconvex, homogeneous, high attenuation extra-axial collection within the right middle cranial fossa (vertical arrow). (b) CT image displayed in “bone window” reveals a fracture of the right greater sphenoid wing (horizontal arrow). The location suggests that the hematoma is due to disruption of the sphenoparietal sinus Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Presentation with EDH “Textbook” presentation (< 10%-27% have this classic presentation): • brief posttraumatic loss of consciousness (LOC): from initial impact • followed by a “lucid interval” for several hours • then, obtundation, contralateral hemiparesis, ipsilateral pupillary dilatation as a result of mass effect from hematoma Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Presentation with EDH • Deterioration usually occurs over a few hours, but may take days and rarely, weeks (longer intervals may be associated with venous bleeding). • Other presenting findings: headache, vomiting, seizure (may be unilateral), hemi-hyperreflexia + unilateral Babinski sign, and elevated CSF pressure (LP is seldom used any longer). Bradycardia late finding • Contralateral hemiparesis is not uniformly seen, especially with EDH in locations other than laterally over the hemisphere Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Differential diagnosis • Subdural hematoma • A posttraumatic disorder described by denny-brown consisting of a “lucid interval” followed by bradycardia, brief periods of restlessness and vomiting, without intracranial hypertension or mass. Children especially may have H/A, and may become drowsy and confused. Theory: a form of vagal syncope. CT must be done to rule out EDH. • Intracranial abscess • Intracranial mass • Seizure • Transient ischemic attack Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Evaluation : Plain Skull X-Ray • Usually not helpful. No fracture is identified in 40% of EDH. In these cases the patient’s age was almost always < 30 yrs. Fissure through the right parietal bone accompanied by small epidural hematoma. Thin fissure through the left parietal and occipital bone. Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
CT scan in EDH • “Classic” CT appearance occurs in 84% of cases: high density biconvex (lenticular) shape adjacent to the skull • In 11% the side against the skull is convex and that along the brain is straight, and in 5% it is crescent shaped (resembling subdural hematoma). • An EDH may cross the falx (distinct from SDH, which is limited to one side of the falx) but is usually limited by skull sutures. Right-sided epidural hematoma. Epidural hematoma (EDH) appears as biconvex (lenticular) shaped hyperdensity adjacent to inner table of skull. Note the underlying skull fracture seen on bone windows. Axial CT scan. A: brain windows. B: bone windows. Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
CT scan in EDH • EDH usually has uniform density, sharply defined edges on multiple cuts, high attenuation (undiluted blood), is contiguous with inner table, and is usually confined to small segment of calvaria. • Mass effect is frequent. • Occasionally, an epidural may be isodense with brain and may not show up unless IV contrast is given. • Mottling of density has been described as a finding in hyperacute EDH. Right-sided epidural hematoma. Epidural hematoma (EDH) appears as biconvex (lenticular) shaped hyperdensity adjacent to inner table of skull. Note the underlying skull fracture seen on bone windows. Axial CT scan. A: brain windows. B: bone windows. Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Management • Management includes: admit, observe (in monitored bed if possible). • Optional: steroids for several days, then taper. • Follow-up CT: in 1 wk if clinically stable. Repeat in 1–3 mos if patient becomes asymptomatic (to document resolution). • Prompt surgery if signs of local mass effect, signs of herniation (increasing drowsiness, pupil changes, hemiparesis), or cardiorespiratory abnormalities. Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Surgical Management : Surgical indications and timing : Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Surgical Management : Surgical technical issues Evacuation is performed in the O.R. unless the patient herniates in E/R and access to OR is not within acceptable timeframe. Objectives: • clot removal: lowers ICP and eliminates focal mass effect. Blood is usually thick coagulum, thus exposure must provide access to most of clot. Craniotomy permits more complete evacuation of hematoma than e.g. burr holes • hemostasis: coagulate bleeding soft tissue (dural veins & arteries). Apply bone wax to intra-diploic bleeders (e.g. middle meningeal artery). Also requires large exposure • prevent reaccumulation: (some bleeding may recur, and dura is now detached from inner table) place dural tack-up sutures to edges of craniotomy and use central “tenting” suture Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Surgical Management Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Special Cases Of Epidural Hematoma Delayed epidural hematoma (DEDH) Posterior fossa epidural hematoma Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Delayed epidural hematoma (DEDH) • Definition: an EDH that is not present on the initial CT scan, but is found on subsequent CT. • Comprise 9–10% of all EDHs in several series • Theoretical risk factors for DEDH include : coagulopathies, lowering ICP, rapidly correcting shock (hemodynamic “surge”) • DEDH tend to occur in patients with severe head injury and associated systemic injuries • Key to diagnosis: high index of suspicion. Avoid a false sense of security imparted by an initial “nonsurgical” CT Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Posterior fossa epidural hematoma • Comprise ≈ 5% of EDH. • More common in 1st two decades of life. • Although as many as 84% have occipital skull fractures, only ≈ 3% of children with occipital skull fractures develop p-fossa EDH. • The source of bleeding is usually not found, but there is a high incidence of tears of the dural sinuses. • Cerebellar signs are surprisingly lacking or subtle in most. • Overall mortality is ≈ 26% (mortality was higher in patients with an associated intracranial lesion) Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Craniotomy for acute EDH/SDH Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Complication • Mass effect: compression of the brain if bleeding is significant • Herniation • Seizures Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Prognosis • In general, patients with pure EDHs have an excellent prognosis of a functional outcome after the surgical evacuation, when it is rapidly detected and evacuated. A delay in diagnosis and treatment increases morbidity and mortality. • EDHs caused by arterial bleeding develop rapidly and can be detected quickly. But those due to a dural sinus tear develop more slowly. Thus, clinical manifestations may be delayed, with a resultant delay in recognition and evacuation. Generally, an EDH volume greater than 50 cm prior to evacuation results in a worse neurological outcome and consequent mortality. Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252
Prognosis Factors that may influence the outcome are as follows: • Patient age • Time lapsed between injury and treatment • Immediate coma or lucid interval • Presence of pupillary abnormalities • GCS/motor score, on arrival Greenberg, Mark S. (2019). Handbook of Neurosurgery. Thieme, New York. Ch. 13, 243 – 252